

Efficiency of laparoscopic retroperitoneal pancreatic necrosectomy for treating infected pancreatic necrosis with duodenal fistula: a single-center retrospective cohort study
- PMID: 39730999
- PMCID: PMC11673563
- DOI: 10.1186/s12876-024-03539-7
Efficiency of laparoscopic retroperitoneal pancreatic necrosectomy for treating infected pancreatic necrosis with duodenal fistula: a single-center retrospective cohort study
Abstract
Background: Open surgical debridement was the main treatment option for infected pancreatic necrosis (IPN). However, it was associated with significant trauma, leading to a higher mortality rate. With the development of minimally invasive surgery, the step-up treatment principle centered around minimally invasive intervention, significantly reducing the incidence of complications and mortality rates among IPN patients. However, few studies have reported the efficacy of laparoscopic retroperitoneal pancreatic necrosectomy (LRPN), a new minimally invasive debridement technique, in IPN patients with duodenal fistula (DF)-a severe complication of IPN. Therefore, we analyzed the effectiveness and safety of LRPN for treating IPN with DF and discussed the impact of DF on patient prognosis.
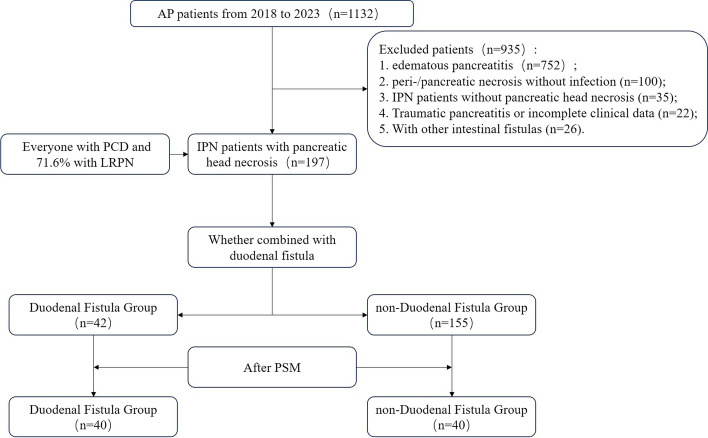
Methods: We retrospectively examined patients diagnosed with IPN between 2018 and 2023. The patients were divided into two groups based on the presence or absence of DF. Clinical characteristics, treatment strategies, clinical outcomes, and follow-up information were analyzed. A 1:1 propensity score-matching (PSM) method was used to assess differences in outcome indicators more accurately.
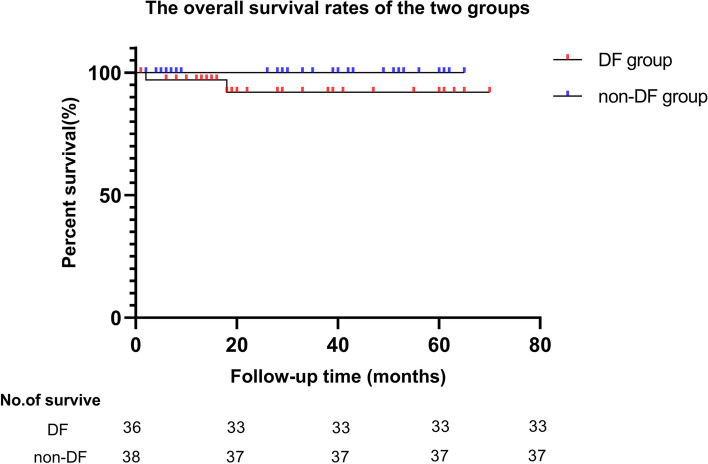
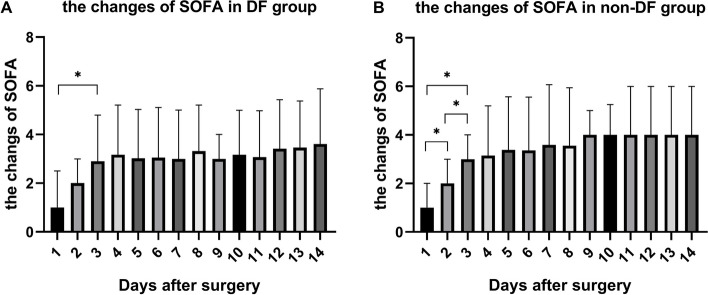
Results: A total of 197 patients were examined. After PSM, no significant differences were observed between the two groups in in-hospital mortality rate, incidence of single organ failure, rate of postoperative severe complications (Clavien-Dindo Classification ≥ 3), and intensive care unit stay (P > 0.05). However, the incidence of multiorgan failure, gastrointestinal bleeding, number of percutaneous catheter drainage (PCD) procedures, surgery cases, hospital stay, and hospitalization costs were higher in the DF group (P < 0.05). Of these patients, 71.6% (n = 141) were treated with PCD + LRPN, with a conversion rate of 6.38% to open surgery. A higher proportion of patients in the non-DF group showed improved clinical outcomes solely with PCD (22.6% vs. 2.4%, P < 0.05), whereas a higher proportion of patients in the DF group underwent PCD + LRPN (88.1% vs. 67.1%, P < 0.05). Both groups showed a significant reduction in the Sequential Organ Failure Assessment score 72 h postoperatively.
Conclusions: For patients with IPN and DF, the LRPN-centered step-up strategy was safe and effective. DF prolongs hospital stay and increases hospitalization costs for patients.
Keywords: Duodenal fistula; Infected necrotizing pancreatitis; Laparoscopic retroperitoneal pancreatic necrosectomy; Propensity score matching.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Sir Run Run Shaw Hospital Ethics Committee (No. 2024–0214). The clinical data of all enrolled patients were obtained from the clinical information system and analyzed anonymously, and the informed consents were waived approved by the ethics committees of the Sir Run Run Shaw Hospital. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
[Comparison of short-term outcomes of robotic and laparoscopic surgery for mid-low rectal cancer: a propensity matched analysis].Zhonghua Wei Chang Wai Ke Za Zhi. 2024 Dec 25;27(12):1261-1268. doi: 10.3760/cma.j.cn441530-20240130-00050. Zhonghua Wei Chang Wai Ke Za Zhi. 2024. PMID: 39710453 Chinese.
-
Sinonasal debridement versus no debridement for the postoperative care of patients undergoing endoscopic sinus surgery.Cochrane Database Syst Rev. 2018 Nov 8;11(11):CD011988. doi: 10.1002/14651858.CD011988.pub2. Cochrane Database Syst Rev. 2018. PMID: 30407624 Free PMC article.
-
Propensity matched analysis of minimally invasive and open radical resection for rectal cancer: comparison of short-term outcomes in elderly/frail patients.J Robot Surg. 2024 Mar 11;18(1):117. doi: 10.1007/s11701-024-01883-0. J Robot Surg. 2024. PMID: 38466495
-
Endovascular repair of abdominal aortic aneurysm.Cochrane Database Syst Rev. 2014 Jan 23;2014(1):CD004178. doi: 10.1002/14651858.CD004178.pub2. Cochrane Database Syst Rev. 2014. PMID: 24453068 Free PMC article. Review.
-
Perioperative glycaemic control for people with diabetes undergoing surgery.Cochrane Database Syst Rev. 2023 Aug 1;8(8):CD007315. doi: 10.1002/14651858.CD007315.pub3. Cochrane Database Syst Rev. 2023. PMID: 37526194 Free PMC article. Review.
References
-
- Iannuzzi J, King J, Leong J, Quan J, Windsor J, Tanyingoh D, et al. Global incidence of acute pancreatitis is increasing over time: a systematic review and meta-analysis. Gastroenterology. 2022;162(1):122–34. - PubMed
-
- Mederos M, Reber H, Girgis M. Acute pancreatitis: a review. JAMA. 2021;325(4):382–90. - PubMed
-
- Forsmark C, Vege S, Wilcox C. Acute Pancreatitis. N Engl J Med. 2016;375(20):1972–81. - PubMed
-
- Boxhoorn L, Voermans R, Bouwense S, Bruno M, Verdonk R, Boermeester M, et al. Acute pancreatitis. Lancet (London, England). 2020;396(10252):726–34. - PubMed
-
- Timmerhuis H, van Dijk S, Hollemans R, Umans D, Sperna Weiland C, Besselink M, et al. Perforation and fistula of the gastrointestinal tract in patients with necrotizing pancreatitis: a nationwide prospective cohort. Ann Surg. 2023;278(2):e284–92. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
