

Effectiveness of Casirivimab-Imdevimab and Sotrovimab During a SARS-CoV-2 Delta Variant Surge: A Cohort Study and Randomized Comparative Effectiveness Trial
- PMID: 35834252
- PMCID: PMC10881222
- DOI: 10.1001/jamanetworkopen.2022.20957
Effectiveness of Casirivimab-Imdevimab and Sotrovimab During a SARS-CoV-2 Delta Variant Surge: A Cohort Study and Randomized Comparative Effectiveness Trial
Abstract
Importance: The effectiveness of monoclonal antibodies (mAbs), casirivimab-imdevimab and sotrovimab, is unknown in patients with mild to moderate COVID-19 caused by the SARS-CoV-2 Delta variant.
Objective: To evaluate the effectiveness of mAb against the Delta variant compared with no mAb treatment and to ascertain the comparative effectiveness of casirivimab-imdevimab and sotrovimab.
Design, setting, and participants: This study comprised 2 parallel studies: (1) a propensity score-matched cohort study of mAb treatment vs no mAb treatment and (2) a randomized comparative effectiveness trial of casirivimab-imdevimab and sotrovimab. The cohort consisted of patients who received mAb treatment at the University of Pittsburgh Medical Center outpatient infusion centers and emergency departments from July 14 to September 29, 2021. Participants were patients with a positive SARS-CoV-2 test result who were eligible to receive mAbs according to emergency use authorization criteria.
Exposure: For the trial, patients were randomized to either intravenous casirivimab-imdevimab or sotrovimab according to a system therapeutic interchange policy.
Main outcomes and measures: For the cohort study, risk ratio (RR) estimates for the primary outcome of hospitalization or death by 28 days were compared between mAb treatment and no mAb treatment using propensity score-matched models. For the comparative effectiveness trial, the primary outcome was hospital-free days (days alive and free of hospitalization) within 28 days after mAb treatment, where patients who died were assigned -1 day in a bayesian cumulative logistic model adjusted for treatment location, age, sex, and time. Inferiority was defined as a 99% posterior probability of an odds ratio (OR) less than 1. Equivalence was defined as a 95% posterior probability that the OR was within a given bound.
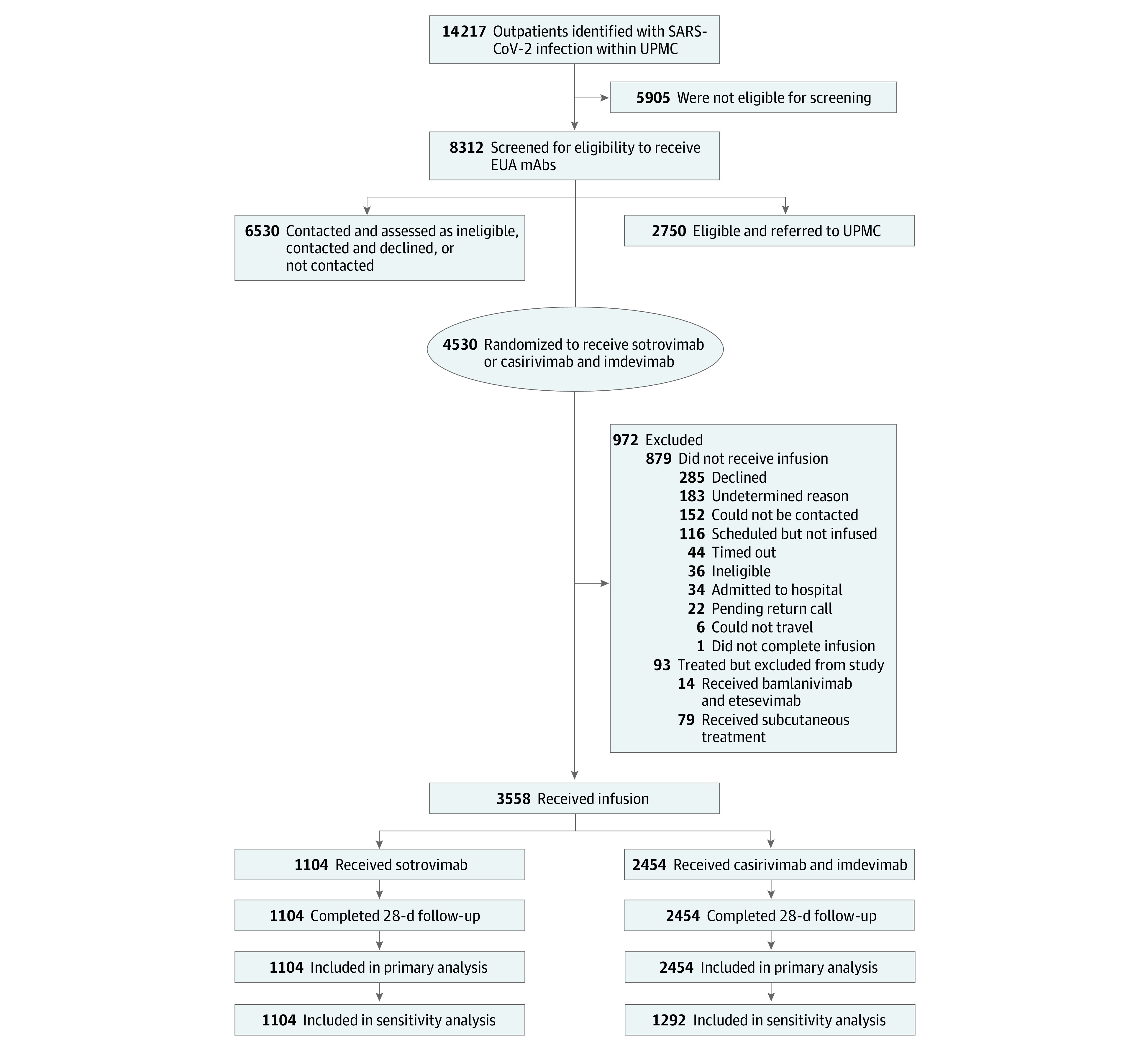
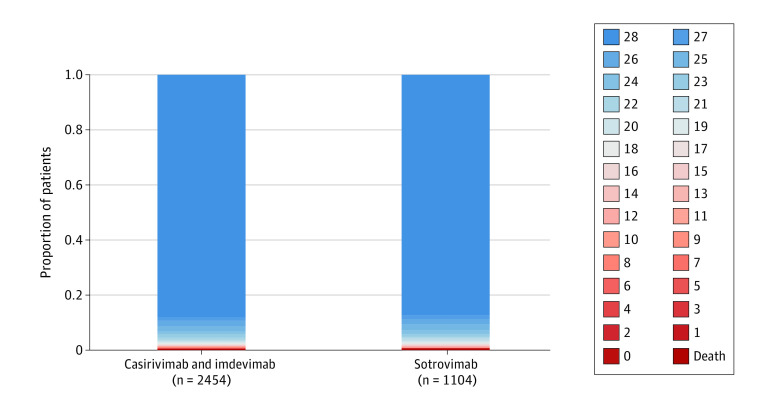
Results: A total of 3069 patients (1023 received mAb treatment: mean [SD] age, 53.2 [16.4] years; 569 women [56%]; 2046 had no mAb treatment: mean [SD] age, 52.8 [19.5] years; 1157 women [57%]) were included in the prospective cohort study, and 3558 patients (mean [SD] age, 54 [18] years; 1919 women [54%]) were included in the randomized comparative effectiveness trial. In propensity score-matched models, mAb treatment was associated with reduced risk of hospitalization or death (RR, 0.40; 95% CI, 0.28-0.57) compared with no treatment. Both casirivimab-imdevimab (RR, 0.31; 95% CI, 0.20-0.50) and sotrovimab (RR, 0.60; 95% CI, 0.37-1.00) were associated with reduced hospitalization or death compared with no mAb treatment. In the clinical trial, 2454 patients were randomized to receive casirivimab-imdevimab and 1104 patients were randomized to receive sotrovimab. The median (IQR) hospital-free days were 28 (28-28) for both mAb treatments, the 28-day mortality rate was less than 1% (n = 12) for casirivimab-imdevimab and less than 1% (n = 7) for sotrovimab, and the hospitalization rate by day 28 was 12% (n = 291) for casirivimab-imdevimab and 13% (n = 140) for sotrovimab. Compared with patients who received casirivimab-imdevimab, those who received sotrovimab had a median adjusted OR for hospital-free days of 0.88 (95% credible interval, 0.70-1.11). This OR yielded 86% probability of inferiority for sotrovimab vs casirivimab-imdevimab and 79% probability of equivalence.
Conclusions and relevance: In this propensity score-matched cohort study and randomized comparative effectiveness trial, the effectiveness of casirivimab-imdevimab and sotrovimab against the Delta variant was similar, although the prespecified criteria for statistical inferiority or equivalence were not met. Both mAb treatments were associated with a reduced risk of hospitalization or death in nonhospitalized patients with mild to moderate COVID-19 caused by the Delta variant.
Trial registration: ClinicalTrials.gov Identifier: NCT04790786.
Conflict of interest statement
Figures
Similar articles
-
The comparative effectiveness of COVID-19 monoclonal antibodies: A learning health system randomized clinical trial.Contemp Clin Trials. 2022 Aug;119:106822. doi: 10.1016/j.cct.2022.106822. Epub 2022 Jun 11. Contemp Clin Trials. 2022. PMID: 35697146 Free PMC article. Clinical Trial.
-
Association of Subcutaneous or Intravenous Administration of Casirivimab and Imdevimab Monoclonal Antibodies With Clinical Outcomes in Adults With COVID-19.JAMA Netw Open. 2022 Apr 1;5(4):e226920. doi: 10.1001/jamanetworkopen.2022.6920. JAMA Netw Open. 2022. PMID: 35412625 Free PMC article.
-
Curbing the Delta Surge: Clinical Outcomes After Treatment With Bamlanivimab-Etesevimab, Casirivimab-Imdevimab, or Sotrovimab for Mild to Moderate Coronavirus Disease 2019.Mayo Clin Proc. 2022 Sep;97(9):1641-1648. doi: 10.1016/j.mayocp.2022.06.015. Epub 2022 Jun 23. Mayo Clin Proc. 2022. PMID: 36058578 Free PMC article.
-
SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19.Cochrane Database Syst Rev. 2021 Sep 2;9(9):CD013825. doi: 10.1002/14651858.CD013825.pub2. Cochrane Database Syst Rev. 2021. PMID: 34473343 Free PMC article. Review.
-
SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19.Cochrane Database Syst Rev. 2022 Jun 17;6(6):CD014945. doi: 10.1002/14651858.CD014945.pub2. Cochrane Database Syst Rev. 2022. PMID: 35713300 Free PMC article. Review.
Cited by
-
Pathophysiological mechanisms of thrombosis in acute and long COVID-19.Front Immunol. 2022 Nov 16;13:992384. doi: 10.3389/fimmu.2022.992384. eCollection 2022. Front Immunol. 2022. PMID: 36466841 Free PMC article. Review.
-
Clinical Antiviral Efficacy of Remdesivir in Coronavirus Disease 2019: An Open-Label, Randomized Controlled Adaptive Platform Trial (PLATCOV).J Infect Dis. 2023 Nov 11;228(10):1318-1325. doi: 10.1093/infdis/jiad275. J Infect Dis. 2023. PMID: 37470445 Free PMC article. Clinical Trial.
-
Lack of efficacy for sotrovimab use in patients with COVID-19: A meta-analysis.J Infect. 2022 Jul;85(1):e10-e12. doi: 10.1016/j.jinf.2022.04.027. Epub 2022 Apr 21. J Infect. 2022. PMID: 35461909 Free PMC article. No abstract available.
-
Sotrovimab in the treatment of coronavirus disease-2019 (COVID-19): a systematic review and meta-analysis of randomized clinical trials.Naunyn Schmiedebergs Arch Pharmacol. 2024 Dec;397(12):9573-9589. doi: 10.1007/s00210-024-03298-y. Epub 2024 Jul 20. Naunyn Schmiedebergs Arch Pharmacol. 2024. PMID: 39031183 Review.
-
Monoclonal antibodies against SARS-CoV-2 to prevent COVID-19 worsening in a large multicenter cohort.Heliyon. 2024 Aug 13;10(16):e36102. doi: 10.1016/j.heliyon.2024.e36102. eCollection 2024 Aug 30. Heliyon. 2024. PMID: 39247344 Free PMC article.
References
-
- Food and Drug Administration . Fact sheet for health care providers emergency use authorization (EUA) of REGEN-COVTM. November 21, 2020. Accessed July 20, 2021. https://www.fda.gov/media/143894/download
-
- US Food and Drug Administration . Frequently asked questions on the emergency use authorization of sotrovimab. May 26, 2021. Accessed October 13, 2021. https://www.fda.gov/media/149535/download
-
- Institute of Medicine . The learning healthcare system: workshop summary. July 2007. Accessed October 13, 2021. https://pubmed.ncbi.nlm.nih.gov/21452449/
-
- McCreary EK, Bariola JR, Minnier T, et al. . A learning health system randomized trial of monoclonal antibodies for COVID-19. medRxiv. Preprint posted online September 9, 2021. doi:10.1101/2021.09.03.21262551 - DOI
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
