

A dormant TIL phenotype defines non-small cell lung carcinomas sensitive to immune checkpoint blockers
- PMID: 30097571
- PMCID: PMC6086912
- DOI: 10.1038/s41467-018-05032-8
A dormant TIL phenotype defines non-small cell lung carcinomas sensitive to immune checkpoint blockers
Abstract
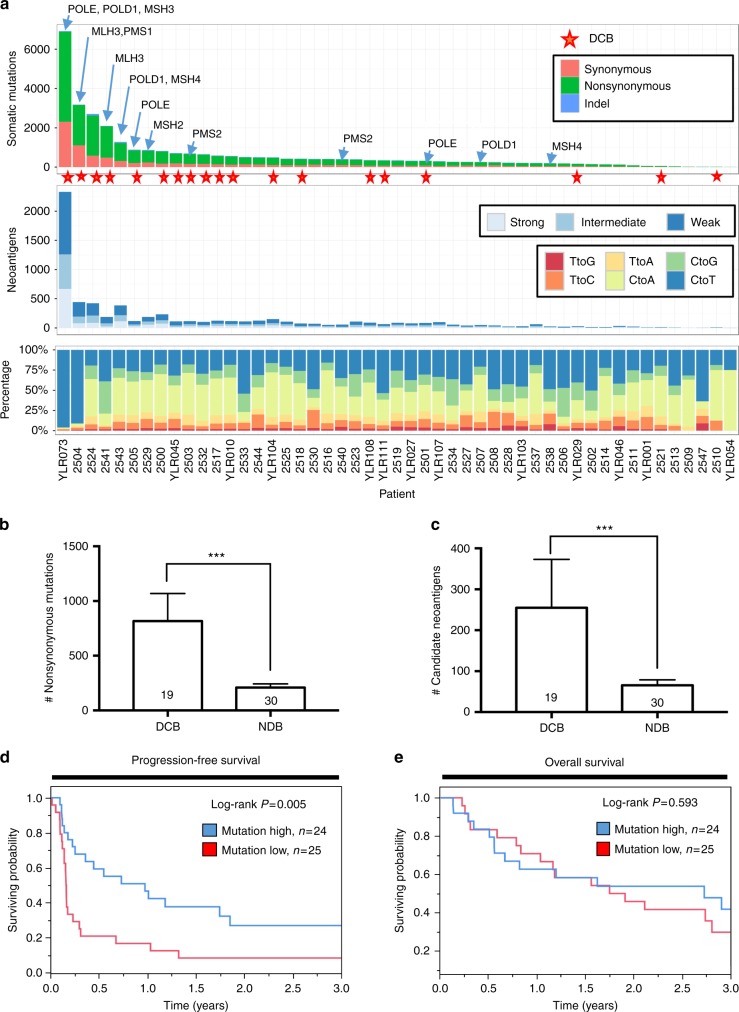
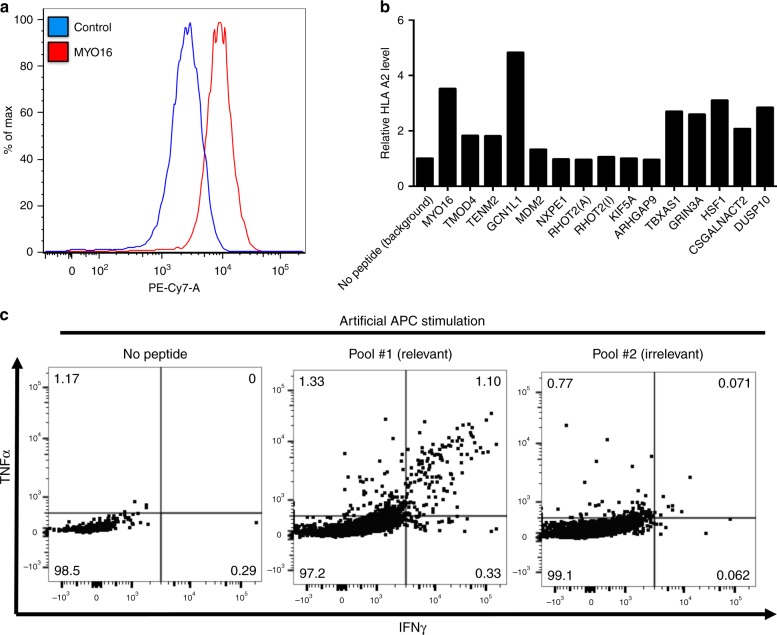
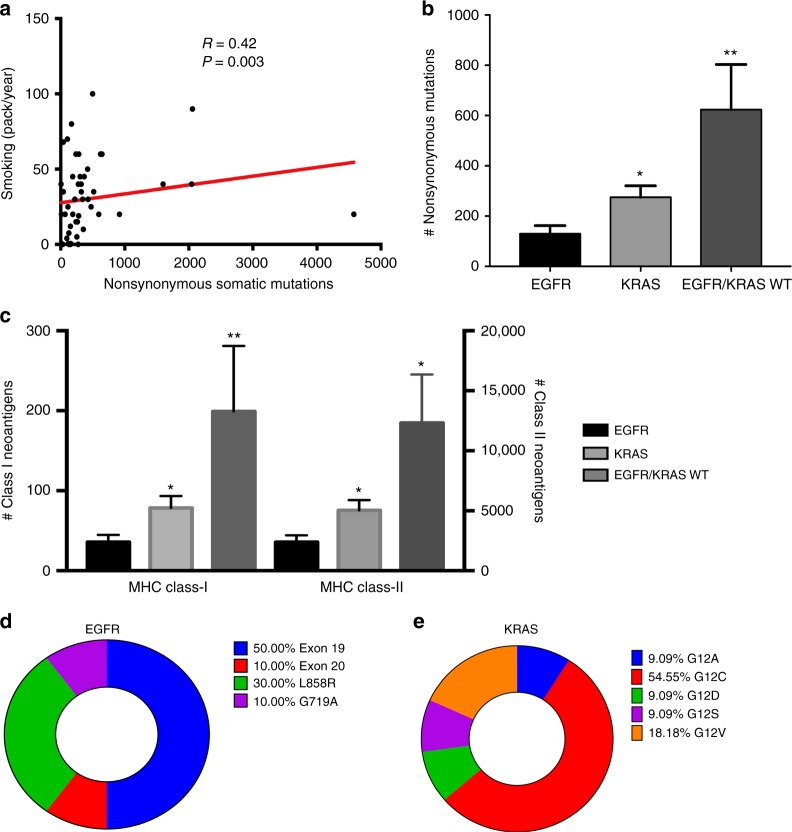
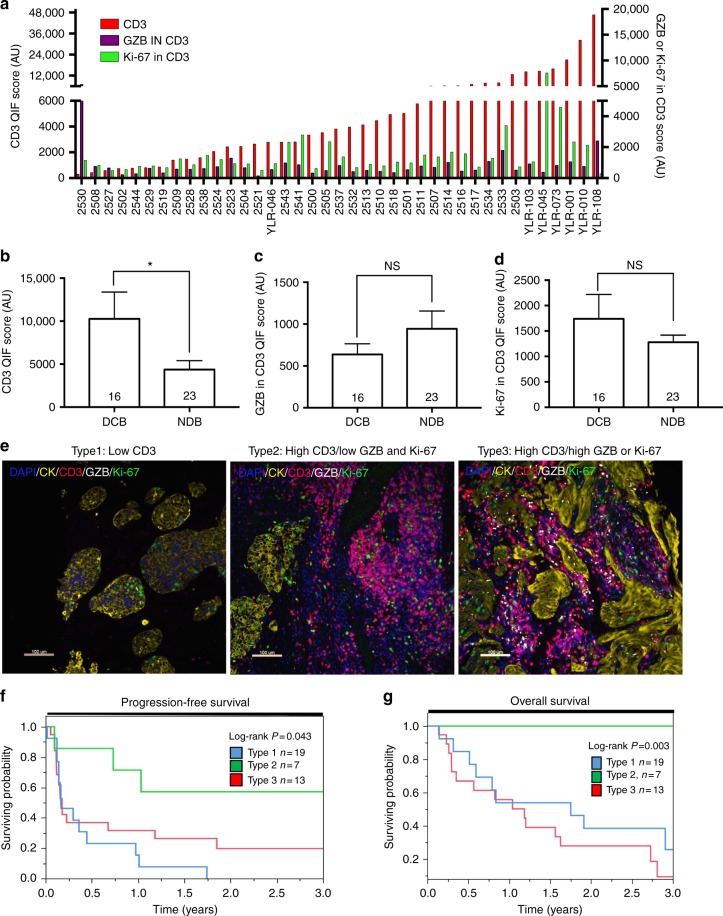
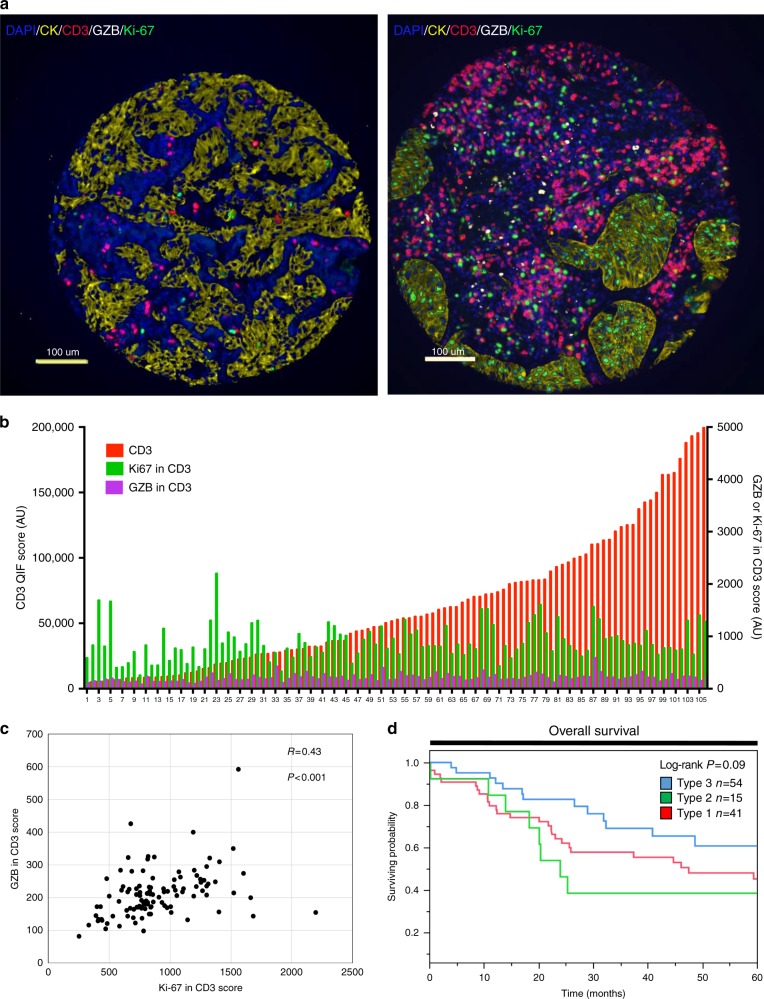
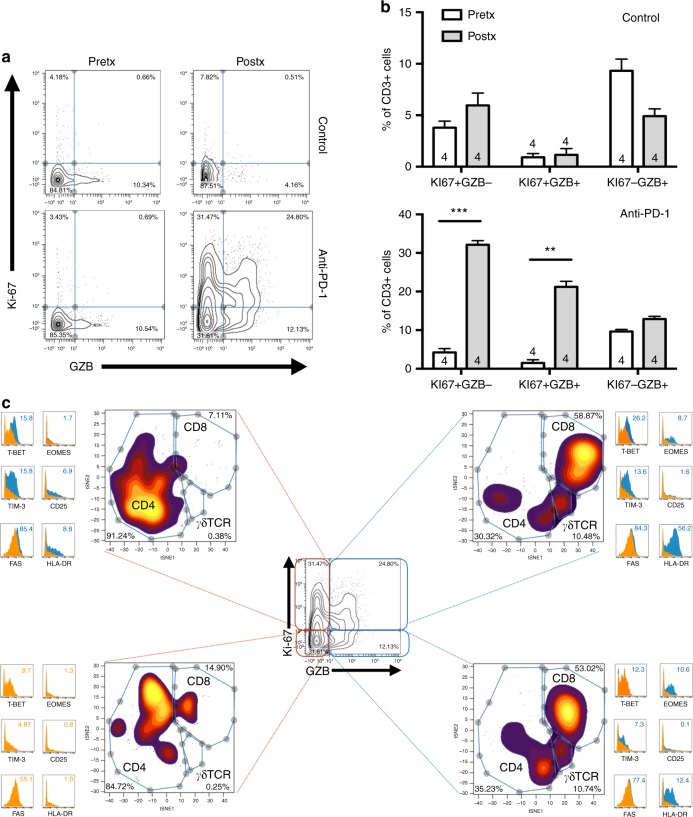
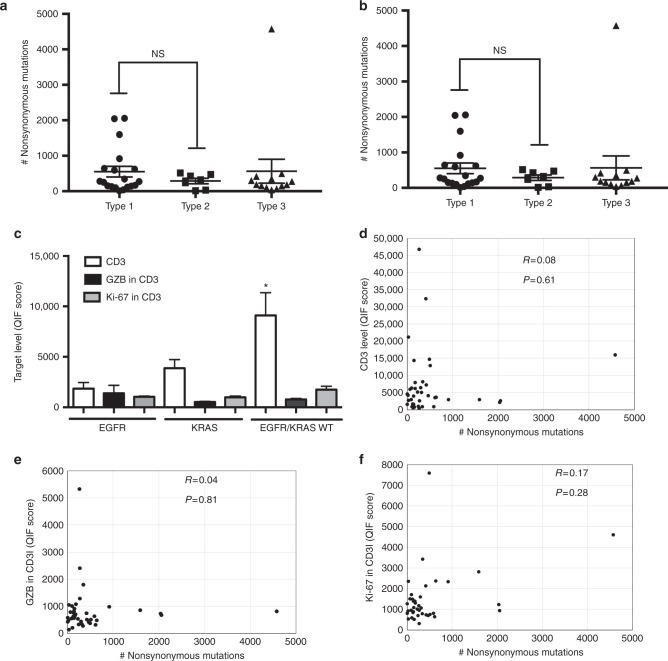
The biological determinants of sensitivity and resistance to immune checkpoint blockers are not completely understood. To elucidate the role of intratumoral T-cells and their association with the tumor genomic landscape, we perform paired whole exome DNA sequencing and multiplexed quantitative immunofluorescence (QIF) in pre-treatment samples from non-small cell lung carcinoma (NSCLC) patients treated with PD-1 axis blockers. QIF is used to simultaneously measure the level of CD3+ tumor infiltrating lymphocytes (TILs), in situ T-cell proliferation (Ki-67 in CD3) and effector capacity (Granzyme-B in CD3). Elevated mutational load, candidate class-I neoantigens or intratumoral CD3 signal are significantly associated with favorable response to therapy. Additionally, a "dormant" TIL signature is associated with survival benefit in patients treated with immune checkpoint blockers characterized by elevated TILs with low activation and proliferation. We further demonstrate that dormant TILs can be reinvigorated upon PD-1 blockade in a patient-derived xenograft model.
Conflict of interest statement
In the last 12 months Dr. Kurt Schalper has been speaker or consultant for Merck, Takeda Pharmaceuticals, Shattuck Labs and Celgene. His laboratory has received research funding from Vasculox/Tioma, Navigate Biopharma, Tesaro Inc, Onkaido Therapeutics/Moderna, Takeda Pharmaceuticals and Surface Oncology. Dr. David Rimm is consultant or advisor to AstraZeneca, Agendia, Agilent, Biocept, Bristo-Myers-Squibb, Cell Signaling Technology. Cepheid, Merck, Optrascan, Perkinelmer and Ultivue. His laboratory has received research funding from AstraZeneca, Cepheid, Navigate/Novartis, NextCure, Gilead Sciences, Ultivue and Perkinelmer. Dr. Rimm also holds equity in PixelGear. Dr. Katerina Politi serves as consultant or advisor for AstraZeneca, Merck, Novartis and Tocagen. Her laboratory received research funds from AstraZeneca, Roche, Kolltan and Symphogen. Dr. Politi also holds royalties in IP licenced from Memorial Sloan Kettering Cancer Center to Molecular MD. Dr. Sarah Goldberg serves as consultant or advisor for AstraZeneca, Bristol-Myers Squibb, Lilly and Boehringer Ingelheim. She received research support from AstraZeneca. Lieping Chen serves as consultant or advisor for Pfizer, Vcanbio and GenomiCare. He is a scientific founder of NextCure and Tayu Biotech. His laboratory receives research funding from NextCure. The remaining authors declare no competing interests. with the content of this work.
Figures
Similar articles
-
Expression Analysis and Significance of PD-1, LAG-3, and TIM-3 in Human Non-Small Cell Lung Cancer Using Spatially Resolved and Multiparametric Single-Cell Analysis.Clin Cancer Res. 2019 Aug 1;25(15):4663-4673. doi: 10.1158/1078-0432.CCR-18-4142. Epub 2019 May 3. Clin Cancer Res. 2019. PMID: 31053602 Free PMC article.
-
Antigen-Presenting Intratumoral B Cells Affect CD4+ TIL Phenotypes in Non-Small Cell Lung Cancer Patients.Cancer Immunol Res. 2017 Oct;5(10):898-907. doi: 10.1158/2326-6066.CIR-17-0075. Epub 2017 Aug 28. Cancer Immunol Res. 2017. PMID: 28848053 Free PMC article.
-
CD8+CD103+ tumor-infiltrating lymphocytes are tumor-specific tissue-resident memory T cells and a prognostic factor for survival in lung cancer patients.J Immunol. 2015 Apr 1;194(7):3475-86. doi: 10.4049/jimmunol.1402711. Epub 2015 Feb 27. J Immunol. 2015. PMID: 25725111
-
Recent Advances in Targeting CD8 T-Cell Immunity for More Effective Cancer Immunotherapy.Front Immunol. 2018 Jan 22;9:14. doi: 10.3389/fimmu.2018.00014. eCollection 2018. Front Immunol. 2018. PMID: 29403496 Free PMC article. Review.
-
The role of B lymphocytes in the immuno-biology of non-small-cell lung cancer.Cancer Immunol Immunother. 2020 Mar;69(3):325-342. doi: 10.1007/s00262-019-02461-2. Epub 2020 Jan 4. Cancer Immunol Immunother. 2020. PMID: 31901949 Free PMC article. Review.
Cited by
-
A novel iTreg-related signature for prognostic prediction in lung adenocarcinoma.Cancer Sci. 2024 Jan;115(1):109-124. doi: 10.1111/cas.16015. Epub 2023 Nov 27. Cancer Sci. 2024. PMID: 38015097 Free PMC article.
-
Tumor cell SYK expression modulates the tumor immune microenvironment composition in human cancer via TNF-α dependent signaling.J Immunother Cancer. 2022 Jul;10(7):e005113. doi: 10.1136/jitc-2022-005113. J Immunother Cancer. 2022. PMID: 35868661 Free PMC article.
-
CCL21-DC in situ vaccination in murine NSCLC overcomes resistance to immunotherapy and generates systemic tumor-specific immunity.J Immunother Cancer. 2023 Sep;11(9):e006896. doi: 10.1136/jitc-2023-006896. J Immunother Cancer. 2023. PMID: 37730274 Free PMC article.
-
Genomic and transcriptomic analysis of checkpoint blockade response in advanced non-small cell lung cancer.Nat Genet. 2023 May;55(5):807-819. doi: 10.1038/s41588-023-01355-5. Epub 2023 Apr 6. Nat Genet. 2023. PMID: 37024582 Free PMC article.
-
KIR3DL3-HHLA2 is a human immunosuppressive pathway and a therapeutic target.Sci Immunol. 2021 Jul 9;6(61):eabf9792. doi: 10.1126/sciimmunol.abf9792. Sci Immunol. 2021. PMID: 34244312 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
