

Controlled direct effects of preeclampsia on neonatal health after accounting for mediation by preterm birth
- PMID: 25437315
- PMCID: PMC6198799
- DOI: 10.1097/EDE.0000000000000213
Controlled direct effects of preeclampsia on neonatal health after accounting for mediation by preterm birth
Abstract
Background: Preeclampsia is characterized by alterations in angiogenic factors that may increase neonatal morbidity independent of preterm birth.
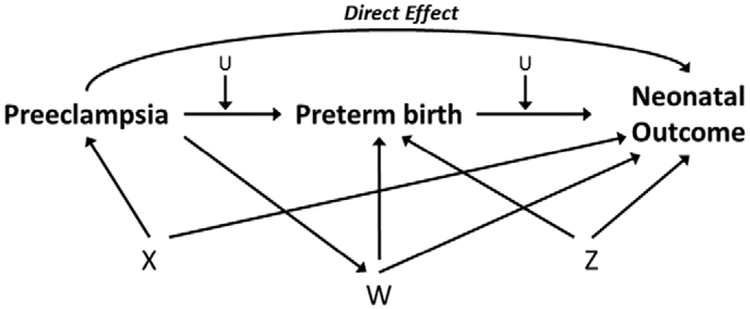
Methods: We estimated the controlled direct effect of preeclampsia on neonatal outcomes independent of preterm birth among 200,103 normotensive and 10,507 preeclamptic singleton pregnancies in the Consortium on Safe Labor (2002-2008). Marginal structural models with stabilized inverse probability weights accounted for potential confounders in the pathway from preeclampsia to preterm birth to neonatal outcomes, including mediator-outcome confounders related to preeclampsia status, such as cesarean delivery. Controlled direct effects of preeclampsia on perinatal mortality, small for gestational age (SGA), neonatal intensive care unit (NICU) admission, respiratory distress syndrome, transient tachypnea of the newborn, anemia, apnea, asphyxia, peri- or intraventricular hemorrhage, and cardiomyopathy were estimated for the hypothesized intervention of term delivery for all infants.
Results: When delivery was set at ≥37 weeks, preeclampsia increased the odds of perinatal mortality (odds ratio = 2.2 [95% confidence interval = 1.1-4.5], SGA = (1.9 [1.8-2.1]), NICU admission (1.9 [1.7-2.1]), respiratory distress syndrome (2.8 [2.0-3.7], transient tachypnea of the newborn (1.6 [1.3-1.9]), apnea (2.2 [1.6-3.1]), asphyxia (2.7 [1.5-4.9]), and peri- or intraventricular hemorrhage (3.2 [1.4-7.7]). No direct effect of preeclampsia at term was observed for anemia or cardiomyopathy. Our results appear robust in the presence of moderate confounding, and restriction to severe preeclampsia yielded similar findings.
Conclusion: Preeclampsia was directly associated with adverse neonatal outcomes beyond morbidity mediated by preterm birth. Although severe neonatal outcomes were less common at later gestational ages, marginal structural models suggested elevated neonatal risk due to preeclampsia even if it was possible to deliver all infants at term.
Figures
Comment in
-
Commentary: from estimation to translation: interpreting mediation analysis results in perinatal epidemiology.Epidemiology. 2015 Jan;26(1):27-9. doi: 10.1097/EDE.0000000000000212. Epidemiology. 2015. PMID: 25437316 No abstract available.
Similar articles
-
Commentary: from estimation to translation: interpreting mediation analysis results in perinatal epidemiology.Epidemiology. 2015 Jan;26(1):27-9. doi: 10.1097/EDE.0000000000000212. Epidemiology. 2015. PMID: 25437316 No abstract available.
-
Neonatal health of infants born to mothers with asthma.J Allergy Clin Immunol. 2014 Jan;133(1):85-90.e1-4. doi: 10.1016/j.jaci.2013.06.012. Epub 2013 Aug 3. J Allergy Clin Immunol. 2014. PMID: 23916153 Free PMC article.
-
Effect of obesity on neonatal outcomes in pregnancies with preterm premature rupture of membranes.Am J Obstet Gynecol. 2016 Feb;214(2):287.e1-287.e5. doi: 10.1016/j.ajog.2015.09.093. Epub 2015 Oct 3. Am J Obstet Gynecol. 2016. PMID: 26435047
-
Consequences of early-onset preeclampsia on neonatal morbidity and mortality.Minerva Pediatr (Torino). 2023 Feb;75(1):87-97. doi: 10.23736/S2724-5276.22.06714-3. Epub 2022 Apr 4. Minerva Pediatr (Torino). 2023. PMID: 35373936 Review.
-
Low-Dose Aspirin for the Prevention of Morbidity and Mortality From Preeclampsia: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2014 Apr. Report No.: 14-05207-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2014 Apr. Report No.: 14-05207-EF-1. PMID: 24783270 Free Books & Documents. Review.
Cited by
-
Genome-Wide Mapping of 5mC and 5hmC Identified Differentially Modified Genomic Regions in Late-Onset Severe Preeclampsia: A Pilot Study.PLoS One. 2015 Jul 27;10(7):e0134119. doi: 10.1371/journal.pone.0134119. eCollection 2015. PLoS One. 2015. PMID: 26214307 Free PMC article.
-
Mediation of Firearm Violence and Preterm Birth by Pregnancy Complications and Health Behaviors: Addressing Structural and Postexposure Confounding.Am J Epidemiol. 2020 Aug 1;189(8):820-831. doi: 10.1093/aje/kwaa046. Am J Epidemiol. 2020. PMID: 32219366 Free PMC article.
-
Mother's care-seeking behavior for neonatal danger signs from qualified providers in rural Bangladesh: A generalized structural equation modeling and mediation analysis.Front Pediatr. 2023 Jan 4;10:929157. doi: 10.3389/fped.2022.929157. eCollection 2022. Front Pediatr. 2023. PMID: 36683813 Free PMC article.
-
Three alternative methods to resolve paradoxical associations of exposures before term.Eur J Epidemiol. 2016 Oct;31(10):1011-1019. doi: 10.1007/s10654-016-0175-1. Epub 2016 Jun 20. Eur J Epidemiol. 2016. PMID: 27325162
-
Identification of Extremely Premature Infants at Low Risk for Early-Onset Sepsis.Pediatrics. 2017 Nov;140(5):e20170925. doi: 10.1542/peds.2017-0925. Epub 2017 Oct 5. Pediatrics. 2017. PMID: 28982710 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
