

Mammary analogue secretory carcinoma of salivary gland origin: an update and expanded morphologic and immunohistochemical spectrum of recently described entity
- PMID: 23821207
- PMCID: PMC3712092
- DOI: 10.1007/s12105-013-0455-y
Mammary analogue secretory carcinoma of salivary gland origin: an update and expanded morphologic and immunohistochemical spectrum of recently described entity
Abstract
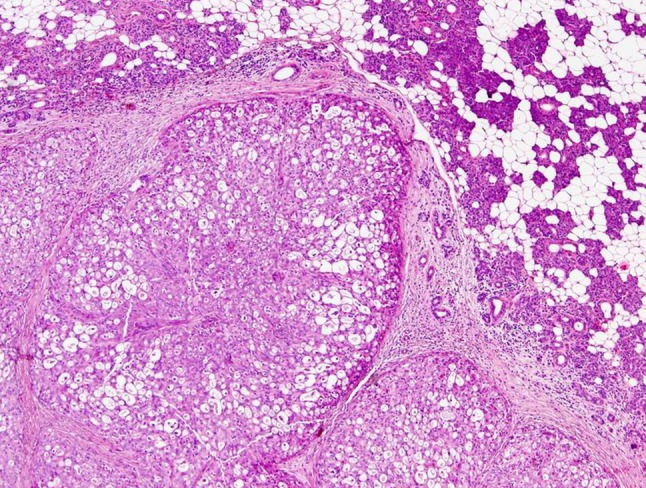
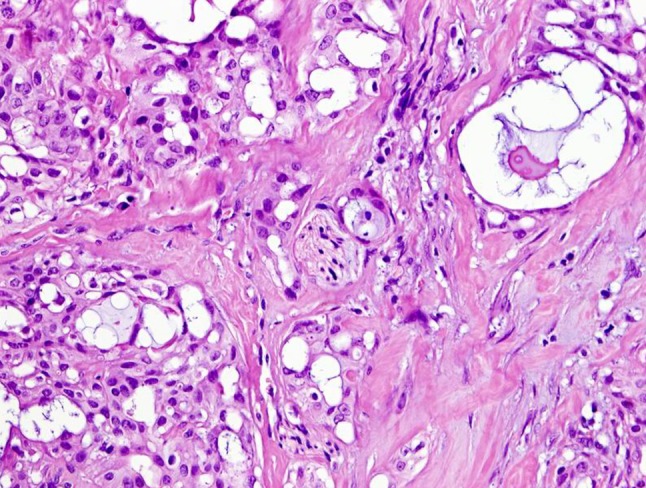
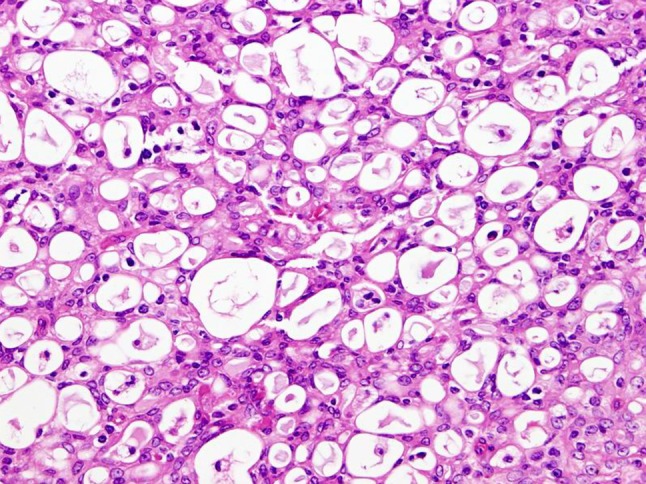
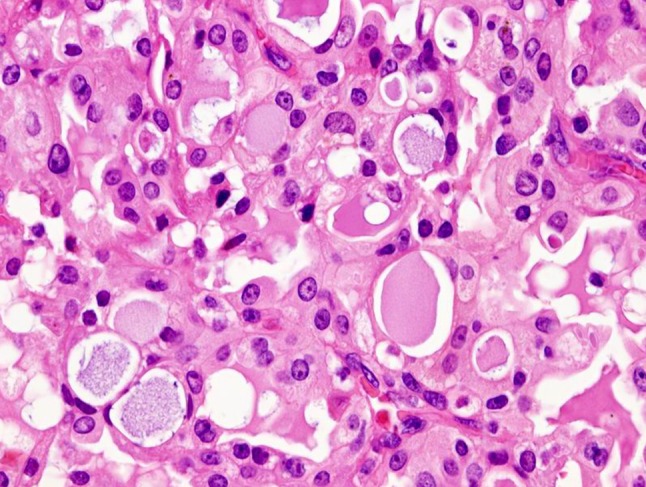
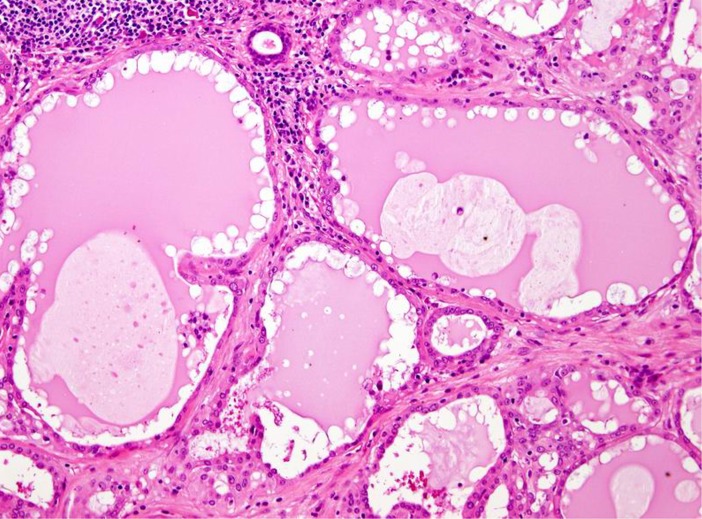
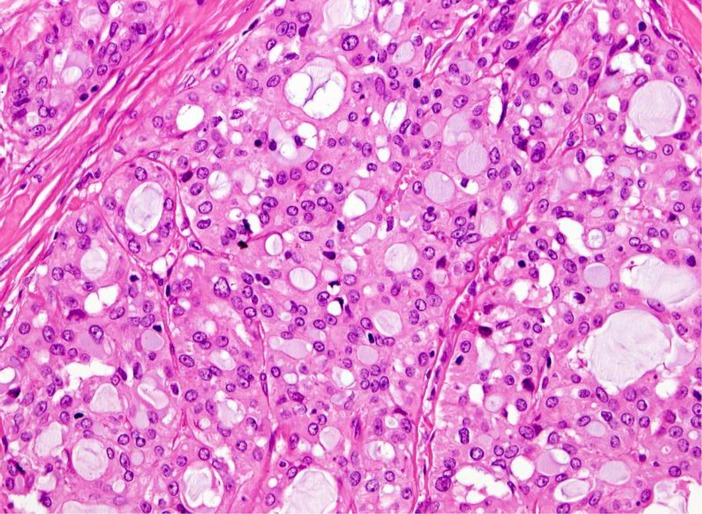
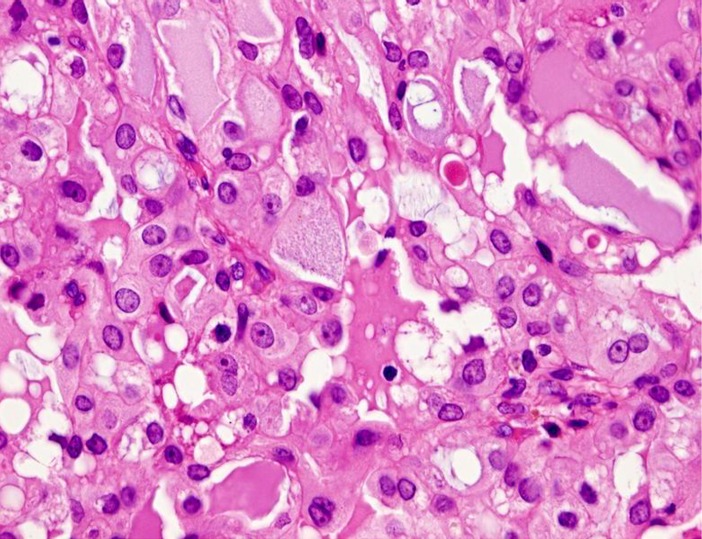
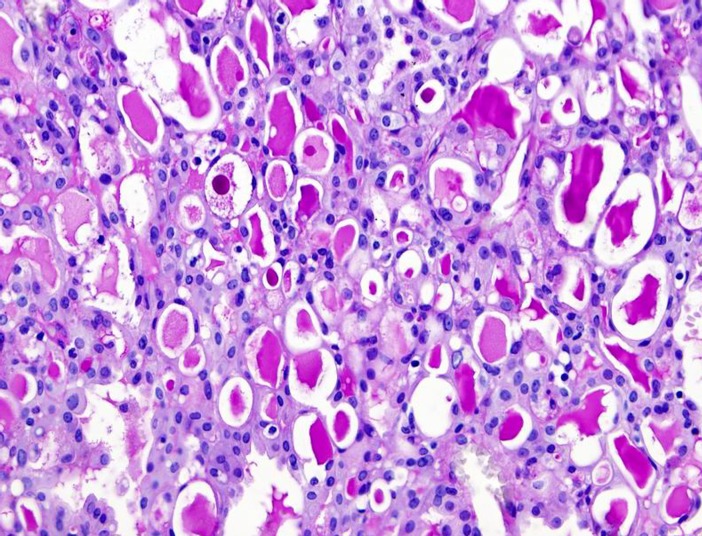
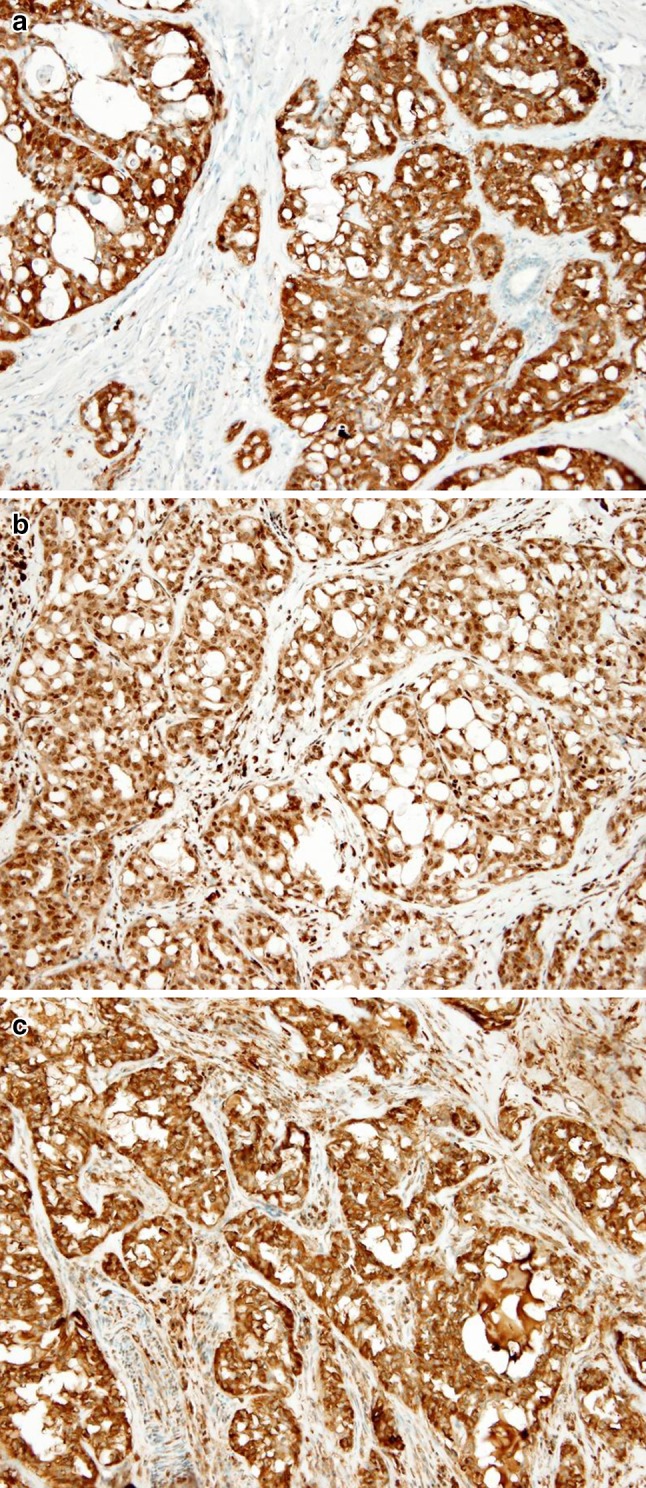
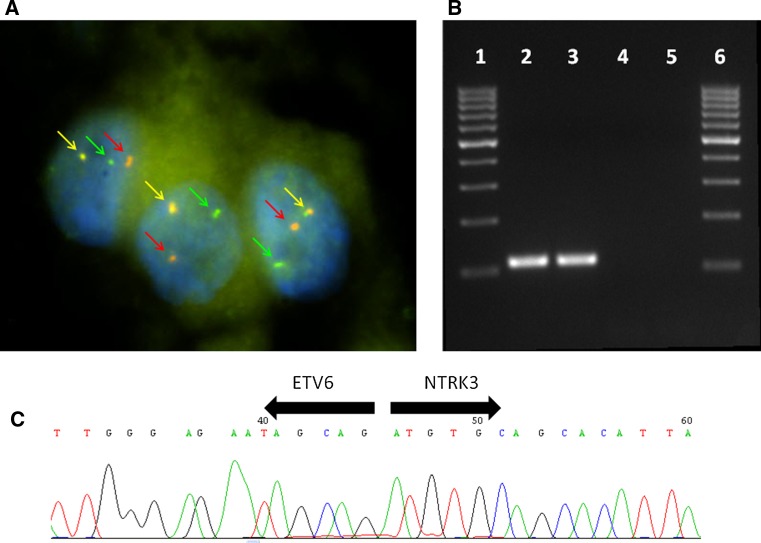
Mammary analogue secretory carcinoma of salivary gland origin (MASC) is a recently described tumor with ETV6 translocation. Akin to secretory breast cancer, MASC expresses S-100 protein, mammaglobin, vimentin, and harbors a t(12;15) (p13;q25) translocation which leads to ETV6-NTRK3 fusion product. Histologically, MASC displays a lobulated growth pattern and is often composed of microcystic, tubular, and solid structures with abundant eosinophilic homogeneous or bubbly secretions. Colloid-like secretory material stains positive for periodic acid-Schiff (PAS) with and without diastase and for Alcian blue. The cells of MASC are devoid of PAS-positive secretory zymogen granules. These features help to exclude the most important differential diagnostic considerations, namely acinic cell carcinoma, low-grade cribriform cystadenocarcinoma, cystadenocarcinoma (not otherwise specified), and low-grade mucoepidermoid carcinoma. To date the presence of the ETV6-NTRK3 fusion gene has not been demonstrated in any other salivary gland tumor than MASC. It is likely that MASC is more common than currently recognized and with further studies, the clinical need for molecular studies of the ETV6-NTRK3 fusion may diminish. However, molecular testing is recommended at this time to arrive at the diagnosis of MASC.
Figures
Similar articles
-
Mammary analog secretory carcinoma of salivary gland origin with the ETV6 gene rearrangement by FISH: expanded morphologic and immunohistochemical spectrum of a recently described entity.Am J Surg Pathol. 2012 Jan;36(1):27-34. doi: 10.1097/PAS.0b013e318231542a. Am J Surg Pathol. 2012. PMID: 21989350
-
Searching for mammary analogue [corrected] secretory carcinoma of salivary gland among its mimics.Mod Pathol. 2014 Jan;27(1):30-7. doi: 10.1038/modpathol.2013.84. Epub 2013 Jun 28. Mod Pathol. 2014. PMID: 23807775
-
Mammary analogue secretory carcinoma of salivary glands with high-grade transformation: report of 3 cases with the ETV6-NTRK3 gene fusion and analysis of TP53, β-catenin, EGFR, and CCND1 genes.Am J Surg Pathol. 2014 Jan;38(1):23-33. doi: 10.1097/PAS.0000000000000088. Am J Surg Pathol. 2014. PMID: 24145651
-
Mammary Analogue Secretory Carcinoma.Arch Pathol Lab Med. 2016 Sep;140(9):997-1001. doi: 10.5858/arpa.2015-0075-RS. Arch Pathol Lab Med. 2016. PMID: 27575269 Review.
-
Mammary analog secretory carcinoma of salivary gland with high-grade histology arising in hard palate, report of a case and review of literature.Int J Clin Exp Pathol. 2014 Dec 1;7(12):9008-22. eCollection 2014. Int J Clin Exp Pathol. 2014. PMID: 25674280 Free PMC article. Review.
Cited by
-
Salivary gland secretory carcinoma presenting as a cervical soft tissue mass: a case report.J Med Case Rep. 2024 Feb 5;18(1):78. doi: 10.1186/s13256-024-04364-y. J Med Case Rep. 2024. PMID: 38311786 Free PMC article. Review.
-
Utility of Immunohistochemistry and ETV6 (12p13) Gene Rearrangement in Identifying Secretory Carcinoma of Salivary Gland among Previously Diagnosed Cases of Acinic Cell Carcinoma.Patholog Res Int. 2017;2017:1497023. doi: 10.1155/2017/1497023. Epub 2017 Apr 6. Patholog Res Int. 2017. PMID: 28484662 Free PMC article.
-
Do not Judge a book by its Cover: A Secretory Carcinoma Arising from a Salivary Gland Heterotopia in Laterocervical lymph-node.Head Neck Pathol. 2024 Oct 22;18(1):109. doi: 10.1007/s12105-024-01708-4. Head Neck Pathol. 2024. PMID: 39436456
-
A Challenging Case of Mammary Analogue Secretory Carcinoma: Case Study with Ultrastructural and Cytogenetic Correlation.Case Rep Pathol. 2019 Dec 17;2019:7468691. doi: 10.1155/2019/7468691. eCollection 2019. Case Rep Pathol. 2019. PMID: 31929931 Free PMC article.
-
Usefulness of immunohistochemistry to distinguish between secretory carcinoma and acinic cell carcinoma in the salivary gland.Med Mol Morphol. 2021 Mar;54(1):23-30. doi: 10.1007/s00795-020-00256-4. Epub 2020 Jun 1. Med Mol Morphol. 2021. PMID: 32488412
References
-
- Barnes L, Eveson J, Reichart P, Sidransky D, editors. Pathology and genetics of head and neck tumours. World Health Organization classification of tumours. Lyon: IARC Press; 2005.
-
- Gnepp DR, Henley JD, Simpson RHW, Eveson J. Salivary and Lacrimal glands. In: Gnepp DR, editors. Diagnostic surgical pathology of the head and neck. 2nd ed. Philadelphia: Saunders Elsevier, pp. 413–562.
-
- Hunt JL. An update on molecular diagnostics of squamous and salivary gland tumors of head and neck. Arch Pathol Lab Med. 2011;135:602–609. - PubMed
-
- McCord C, Weinreb I, Perez-Ordonez B. Progress in salivary gland pathology: new entities and selected molecular features. Diagnostic Histopathol. 2012;18(6):253–260. doi: 10.1016/j.mpdhp.2012.03.005. - DOI
-
- Skalova A, Vanecek T, Simpson RHW, Michal M. Molecular advances in salivary gland pathology and their practical application. Diagnostic Histopathol. 2012;18(9):388–396. doi: 10.1016/j.mpdhp.2012.08.002. - DOI
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
