

Activation of nuclear factor kappa B inflammatory bowel disease
- PMID: 9616307
- PMCID: PMC1727068
- DOI: 10.1136/gut.42.4.477
Activation of nuclear factor kappa B inflammatory bowel disease
Abstract
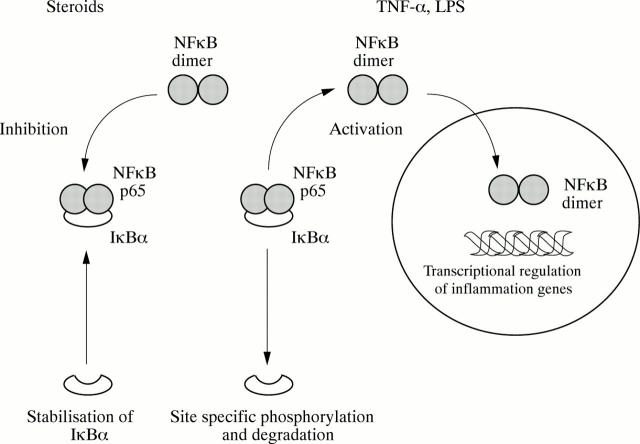
Background: Expression of pro-inflammatory cytokines is increased in the intestinal lamina propria of patients with inflammatory bowel disease (IBD). Nuclear factor kappa B (NF kappa B) controls transcription of inflammation genes. On activation, NF kappa B is rapidly released from its cytoplasmic inhibitor (I kappa B), transmigrates into the nucleus, and binds to DNA response elements in gene promoter regions.
Aims: To investigate whether increased activation of NF kappa B is important in IBD and may be down-regulated by anti-inflammatory treatment.
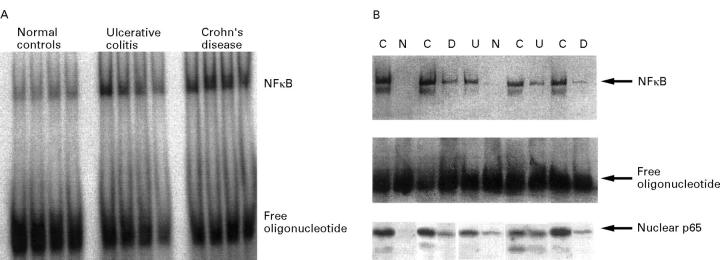
Methods: Activation of NF kappa B was determined by western blot assessment and electrophoretic mobility shift assay in nuclear extracts of colonic biopsy samples as well as lamina propria mononuclear cells.
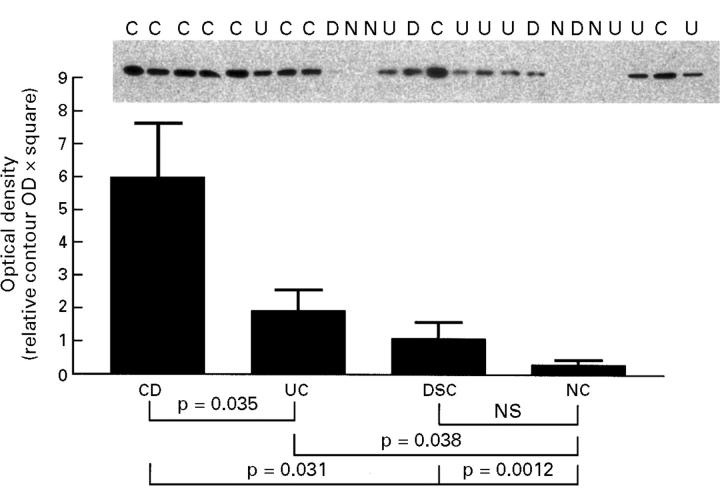
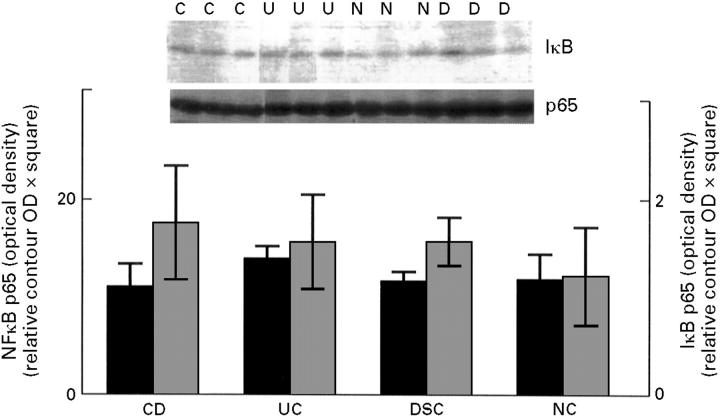
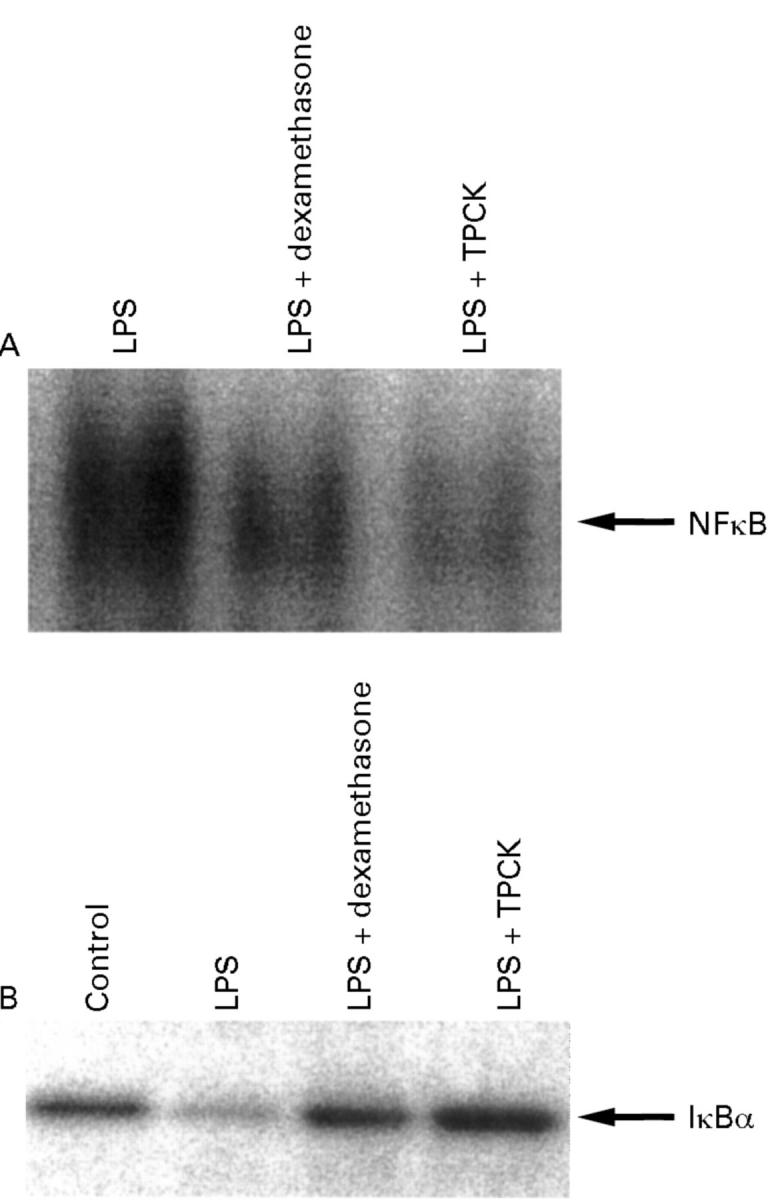
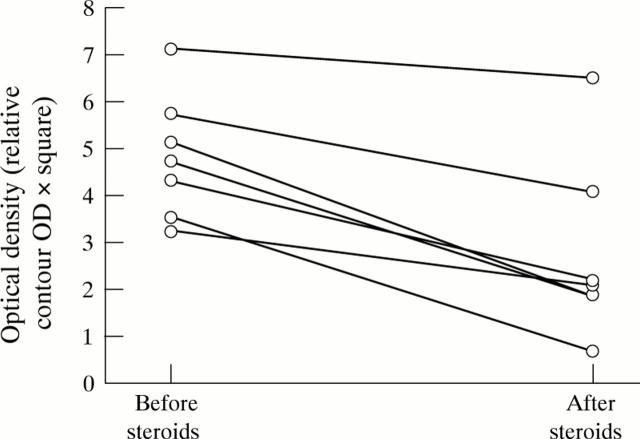
Results: Nuclear levels of NF kappa B p65 are increased in lamina propria biopsy specimens from patients with Crohn's disease in comparison with patients with ulcerative colitis and controls. Increased activation of NF kappa B was detected in lamina propria mononuclear cells from patients with active IBD. Corticosteroids strongly inhibit intestinal NF kappa B activation in IBD in vivo and in vitro by stabilising the cytosolic inhibitor I kappa B alpha against activation induced degradation.
Conclusions: In both IBDs, but particularly Crohn's disease, increased activation of NF kappa B may be involved in the regulation of the inflammatory response. Inhibition of NF kappa B activation may represent a mechanism by which steroids exert an anti-inflammatory effect in IBD.
Figures
Comment in
-
Activation of NFkappaB in inflammatory bowel disease.Gut. 1998 Oct;43(4):587-8. doi: 10.1136/gut.43.4.586c. Gut. 1998. PMID: 9882195 Free PMC article. No abstract available.
Similar articles
-
Cell specific effects of glucocorticoid treatment on the NF-kappaBp65/IkappaBalpha system in patients with Crohn's disease.Gut. 1999 Nov;45(5):693-704. doi: 10.1136/gut.45.5.693. Gut. 1999. PMID: 10517905 Free PMC article.
-
Activation of signal transducer and activator of transcription (STAT) 1 in human chronic inflammatory bowel disease.Gut. 2002 Sep;51(3):379-85. doi: 10.1136/gut.51.3.379. Gut. 2002. PMID: 12171960 Free PMC article.
-
Rho kinase blockade prevents inflammation via nuclear factor kappa B inhibition: evidence in Crohn's disease and experimental colitis.Gastroenterology. 2003 May;124(5):1180-7. doi: 10.1016/s0016-5085(03)00283-x. Gastroenterology. 2003. PMID: 12730857 Clinical Trial.
-
Glucocorticoid resistance in inflammatory bowel disease.J Endocrinol. 2003 Sep;178(3):339-46. doi: 10.1677/joe.0.1780339. J Endocrinol. 2003. PMID: 12967327 Review.
-
Nuclear factor-κB - importance, induction of inflammation, and effects of pharmacological modulators in Crohn's disease.J Physiol Pharmacol. 2020 Aug;71(4). doi: 10.26402/jpp.2020.4.01. Epub 2020 Nov 15. J Physiol Pharmacol. 2020. PMID: 33214334 Review.
Cited by
-
Novel Synthetic Oxazines Target NF-κB in Colon Cancer In Vitro and Inflammatory Bowel Disease In Vivo.PLoS One. 2016 Sep 29;11(9):e0163209. doi: 10.1371/journal.pone.0163209. eCollection 2016. PLoS One. 2016. PMID: 27685808 Free PMC article.
-
Insights from advances in research of chemically induced experimental models of human inflammatory bowel disease.World J Gastroenterol. 2007 Nov 14;13(42):5581-93. doi: 10.3748/wjg.v13.i42.5581. World J Gastroenterol. 2007. PMID: 17948932 Free PMC article. Review.
-
P2Y2 receptor transcription is increased by NF-kappa B and stimulates cyclooxygenase-2 expression and PGE2 released by intestinal epithelial cells.J Immunol. 2009 Oct 1;183(7):4521-9. doi: 10.4049/jimmunol.0803977. Epub 2009 Sep 4. J Immunol. 2009. PMID: 19734210 Free PMC article.
-
Small therapeutic molecules for the treatment of inflammatory bowel disease.Gut. 2002 May;50 Suppl 3(Suppl 3):III47-53. doi: 10.1136/gut.50.suppl_3.iii47. Gut. 2002. PMID: 11953333 Free PMC article. Review.
-
Pro-Inflammatory Effects of NX-3 Toxin Are Comparable to Deoxynivalenol and not Modulated by the Co-Occurring Pro-Oxidant Aurofusarin.Microorganisms. 2020 Apr 21;8(4):603. doi: 10.3390/microorganisms8040603. Microorganisms. 2020. PMID: 32326355 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical