

Preemptive CD8 T-cell immunotherapy of acute cytomegalovirus infection prevents lethal disease, limits the burden of latent viral genomes, and reduces the risk of virus recurrence
- PMID: 9499030
- PMCID: PMC109469
- DOI: 10.1128/JVI.72.3.1797-1804.1998
Preemptive CD8 T-cell immunotherapy of acute cytomegalovirus infection prevents lethal disease, limits the burden of latent viral genomes, and reduces the risk of virus recurrence
Abstract
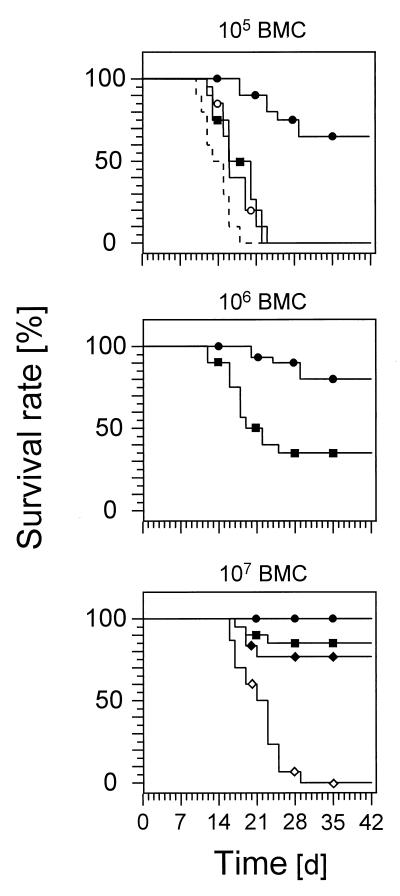
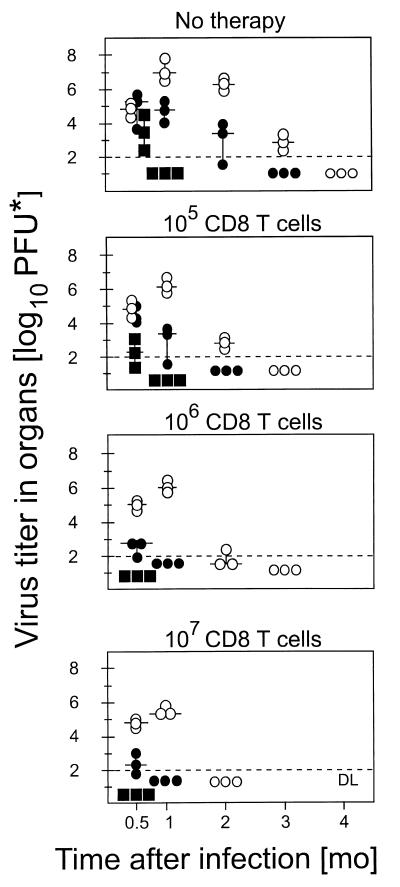
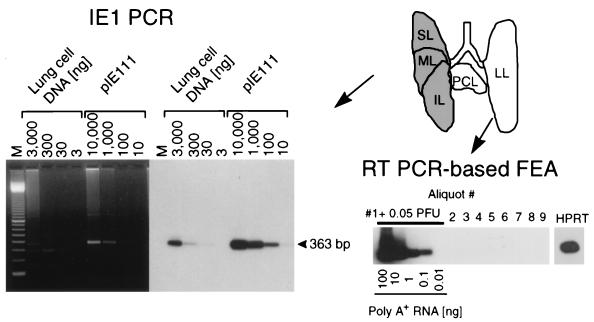
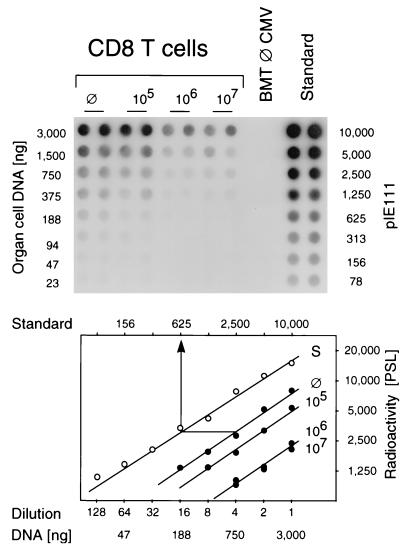
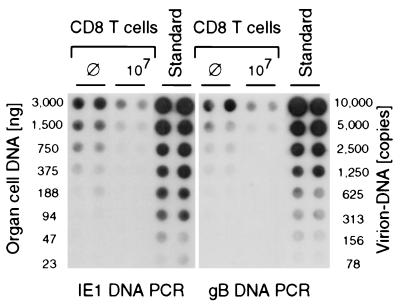
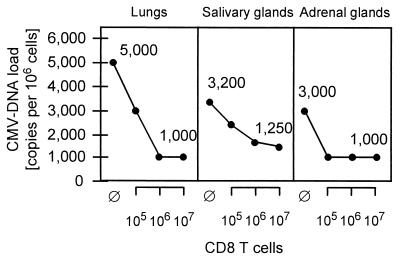
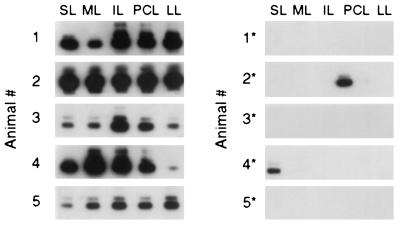
In the immunocompetent host, primary cytomegalovirus (CMV) infection is resolved by the immune response without causing overt disease. The viral genome, however, is not cleared but is maintained in a latent state that entails a risk of virus recurrence and consequent organ disease. By using murine CMV as a model, we have shown previously that multiple organs harbor latent CMV and that reactivation occurs with an incidence that is determined by the viral DNA load in the respective organ (M. J. Reddehase, M. Balthesen, M. Rapp, S. Jonjic, I. Pavic, and U. H. Koszinowski. J. Exp. Med. 179:185-193, 1994). This predicts that a therapeutic intervention capable of limiting the load of latent viral genome should also reduce the risk of virus recurrence. Here we demonstrate the benefits and the limits of a preemptive CD8 T-cell immunotherapy of CMV infection in the immunocompromised bone marrow transplantation recipient. Antiviral CD8 T cells prevented CMV disease and accelerated the resolution of productive infection. The therapy also resulted in a lower load of latent CMV DNA in organs and consequently reduced the incidence of recurrence. The data thus provide a further supporting argument for clinical trials of preemptive cytoimmunotherapy of human CMV disease with CD8 T cells. However, CD8 T cells failed to clear the viral DNA. The therapy-susceptible portion of the DNA load differed between organs and was highest in the lungs. The existence of an invariant, therapy-resistant load suggests a role for immune system evasion mechanisms in the establishment of CMV latency.
Figures
Similar articles
-
The establishment of cytomegalovirus latency in organs is not linked to local virus production during primary infection.J Gen Virol. 1994 Sep;75 ( Pt 9):2329-36. doi: 10.1099/0022-1317-75-9-2329. J Gen Virol. 1994. PMID: 8077931
-
Murine model of interstitial cytomegalovirus pneumonia in syngeneic bone marrow transplantation: persistence of protective pulmonary CD8-T-cell infiltrates after clearance of acute infection.J Virol. 2000 Aug;74(16):7496-507. doi: 10.1128/jvi.74.16.7496-7507.2000. J Virol. 2000. PMID: 10906203 Free PMC article.
-
Pediatric roots of cytomegalovirus recurrence and memory inflation in the elderly.Med Microbiol Immunol. 2019 Aug;208(3-4):323-328. doi: 10.1007/s00430-019-00609-6. Epub 2019 May 6. Med Microbiol Immunol. 2019. PMID: 31062089 Review.
-
Therapeutic Vaccination of Hematopoietic Cell Transplantation Recipients Improves Protective CD8 T-Cell Immunotherapy of Cytomegalovirus Infection.Front Immunol. 2021 Aug 19;12:694588. doi: 10.3389/fimmu.2021.694588. eCollection 2021. Front Immunol. 2021. PMID: 34489940 Free PMC article.
-
Pathogenesis of cytomegalovirus pneumonia in immunocompromised hosts.Semin Respir Infect. 1995 Dec;10(4):199-208. Semin Respir Infect. 1995. PMID: 8668847 Review.
Cited by
-
Enrichment of immediate-early 1 (m123/pp89) peptide-specific CD8 T cells in a pulmonary CD62L(lo) memory-effector cell pool during latent murine cytomegalovirus infection of the lungs.J Virol. 2000 Dec;74(24):11495-503. doi: 10.1128/jvi.74.24.11495-11503.2000. J Virol. 2000. PMID: 11090146 Free PMC article.
-
Refinement of strategies for the development of a human cytomegalovirus dense body vaccine.Med Microbiol Immunol. 2008 Jun;197(2):97-107. doi: 10.1007/s00430-008-0085-2. Epub 2008 Mar 5. Med Microbiol Immunol. 2008. PMID: 18320219
-
Herpesvirus latency and symbiotic protection from bacterial infection.Viral Immunol. 2009 Feb;22(1):3-4; author reply 5-6. doi: 10.1089/vim.2008.0100. Viral Immunol. 2009. PMID: 19210221 Free PMC article. No abstract available.
-
Recombinant viruses as tools to study human cytomegalovirus immune modulation.Med Microbiol Immunol. 2008 Jun;197(2):215-22. doi: 10.1007/s00430-008-0083-4. Epub 2008 Feb 27. Med Microbiol Immunol. 2008. PMID: 18301917 Review.
-
Immune evasion proteins enhance cytomegalovirus latency in the lungs.J Virol. 2009 Oct;83(19):10293-8. doi: 10.1128/JVI.01143-09. Epub 2009 Jul 15. J Virol. 2009. PMID: 19605491 Free PMC article.
References
-
- Balthesen M, Dreher L, Lucin P, Reddehase M J. The establishment of cytomegalovirus latency in organs is not linked to local virus production during primary infection. J Gen Virol. 1994;75:2329–2336. - PubMed
-
- Chun T-W, Carruth L, Finzi D, Shen X, DiGiuseppe J A, Taylor H, Hermankova M, Chadwick K, Margolick J, Quinn T C, Kuo Y-H, Brookmeyer R, Zeiger M A, Barditch-Crovo P, Siliciano R F. Quantification of latent tissue reservoirs and total body viral load in HIV-1 infection. Nature (London) 1997;387:183–188. - PubMed
-
- Cobbold S P, Jayasuriya A, Nash A, Prospero T D, Waldmann H. Therapy with monoclonal antibodies by elimination of T-cell subsets in vivo. Nature (London) 1984;312:548–550. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
