

This is a preprint.
Recent Endemic Coronavirus Infection Associates With Higher SARS-CoV-2 Cross-Reactive Fc Receptor Binding Antibodies
- PMID: 39484477
- PMCID: PMC11527020
- DOI: 10.1101/2024.10.23.619886
Recent Endemic Coronavirus Infection Associates With Higher SARS-CoV-2 Cross-Reactive Fc Receptor Binding Antibodies
Abstract
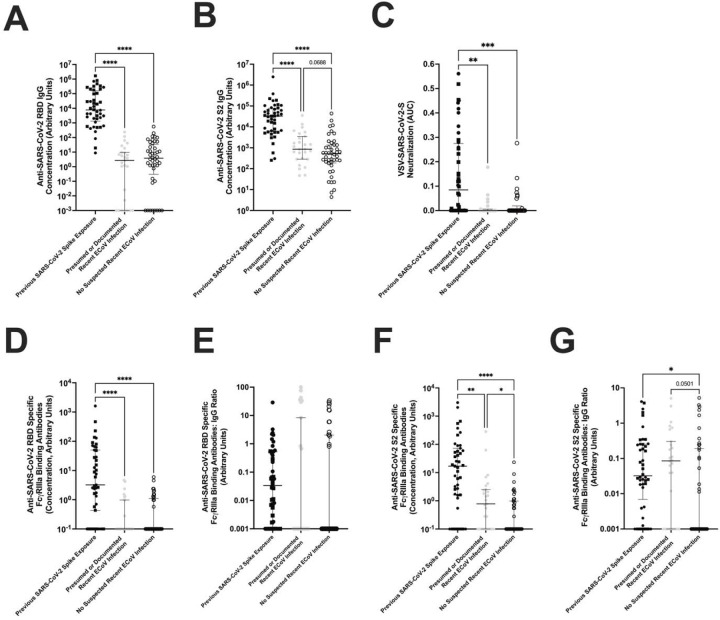
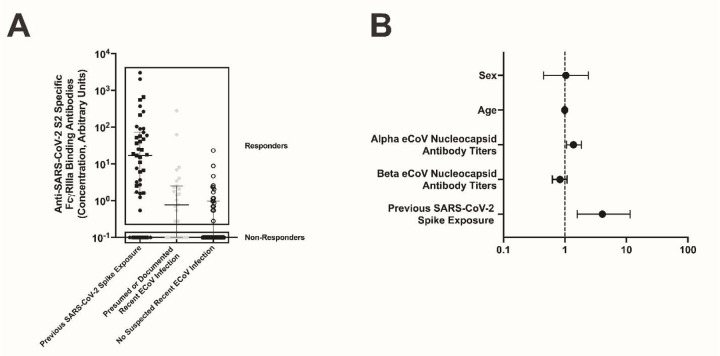
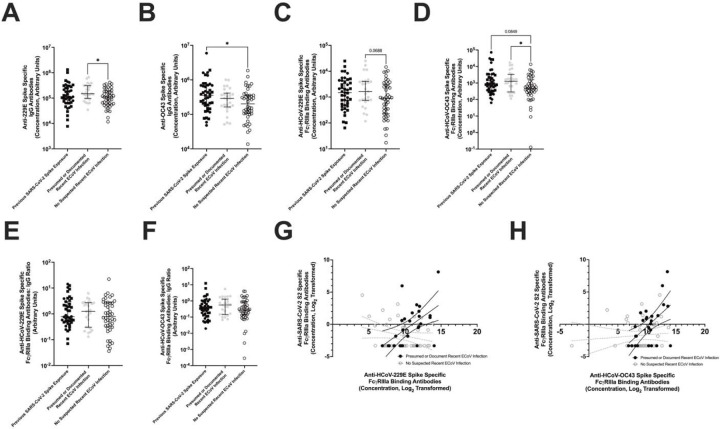
Recent documented infection with an endemic coronavirus (eCoV) associates with less severe coronavirus disease 2019 (COVID-19), yet the immune mechanism behind this protection has not been fully explored. We measured both antibody and T cell responses against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in SARS-CoV-2 naïve individuals classified into two groups, either with or without presumed recent eCoV infections. There was no difference in neutralizing antibodies and T cell responses against SARS-CoV-2 antigens between the two groups. SARS-CoV-2 naïve individuals with recent presumed eCoV infection, however, had higher levels of Fc receptor (FcR) binding antibodies against eCoV spikes (S) and SARS-CoV-2 S2. There was also a significant correlation between eCoV and SARS-CoV-2 FcR binding antibodies. Recent eCoV infection boosts cross-reactive antibodies that can mediate Fc effector functions, and this may play a role in the observed heterotypic immune protection against severe COVID-19.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
Similar articles
-
Heterotypic immunity from prior SARS-CoV-2 infection but not COVID-19 vaccination associates with lower endemic coronavirus incidence.Sci Transl Med. 2024 Jun 12;16(751):eado7588. doi: 10.1126/scitranslmed.ado7588. Epub 2024 Jun 12. Sci Transl Med. 2024. PMID: 38865483 Free PMC article.
-
Heterotypic responses against nsp12/nsp13 from prior SARS-CoV-2 infection associates with lower subsequent endemic coronavirus incidence.bioRxiv [Preprint]. 2023 Oct 24:2023.10.23.563621. doi: 10.1101/2023.10.23.563621. bioRxiv. 2023. Update in: Sci Transl Med. 2024 Jun 12;16(751):eado7588. doi: 10.1126/scitranslmed.ado7588 PMID: 37961343 Free PMC article. Updated. Preprint.
-
Hybrid Immunity Shifts the Fc-Effector Quality of SARS-CoV-2 mRNA Vaccine-Induced Immunity.mBio. 2022 Oct 26;13(5):e0164722. doi: 10.1128/mbio.01647-22. Epub 2022 Aug 24. mBio. 2022. PMID: 36000735 Free PMC article.
-
Single domain antibodies derived from ancient animals as broadly neutralizing agents for SARS-CoV-2 and other coronaviruses.Biomed Eng Adv. 2022 Dec;4:100054. doi: 10.1016/j.bea.2022.100054. Epub 2022 Sep 18. Biomed Eng Adv. 2022. PMID: 36158162 Free PMC article. Review.
-
Cross-Reactive Immune Responses toward the Common Cold Human Coronaviruses and Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Mini-Review and a Murine Study.Microorganisms. 2021 Jul 31;9(8):1643. doi: 10.3390/microorganisms9081643. Microorganisms. 2021. PMID: 34442723 Free PMC article. Review.
References
-
- Edridge AWD, Kaczorowska J, Hoste ACR, Bakker M, Klein M, Loens K, Jebbink MF, Matser A, Kinsella CM, Rueda P, Ieven M, Goossens H, Prins M, Sastre P, Deijs M, van der Hoek L. 2020. Seasonal coronavirus protective immunity is short-lasting. Nat Med 26:1691–1693. - PubMed
-
- Bean DJ, Monroe J, Liang YM, Borberg E, Senussi Y, Swank Z, Chalise S, Walt D, Weinberg J, Sagar M. 2024. Heterotypic immunity from prior SARS-CoV-2 infection but not COVID-19 vaccination associates with lower endemic coronavirus incidence. Sci Transl Med 16:eado7588. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous