

Association between the neutrophil-to-lymphocyte ratio and in-hospital mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit
- PMID: 38689359
- PMCID: PMC11059689
- DOI: 10.1186/s40001-024-01850-3
Association between the neutrophil-to-lymphocyte ratio and in-hospital mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit
Abstract
Background: The objective of this study was to investigate the correlation between neutrophil-to-lymphocyte ratios (NLR) and the risk of in-hospital death in patients admitted to the intensive care unit (ICU) with both chronic kidney disease (CKD) and coronary artery disease (CAD).
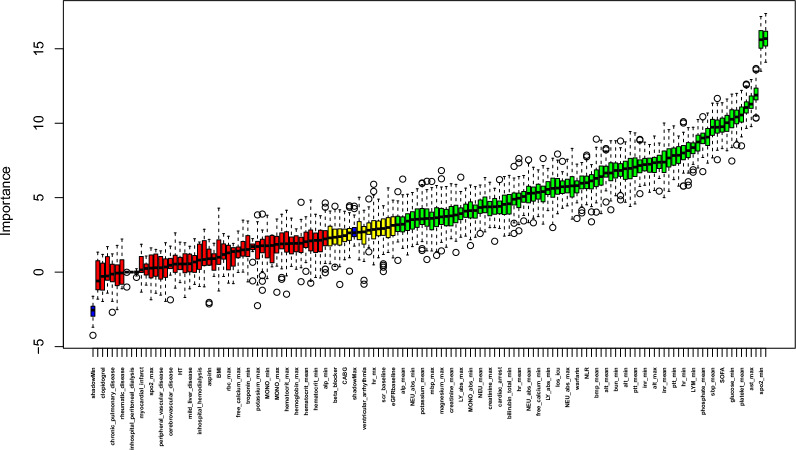
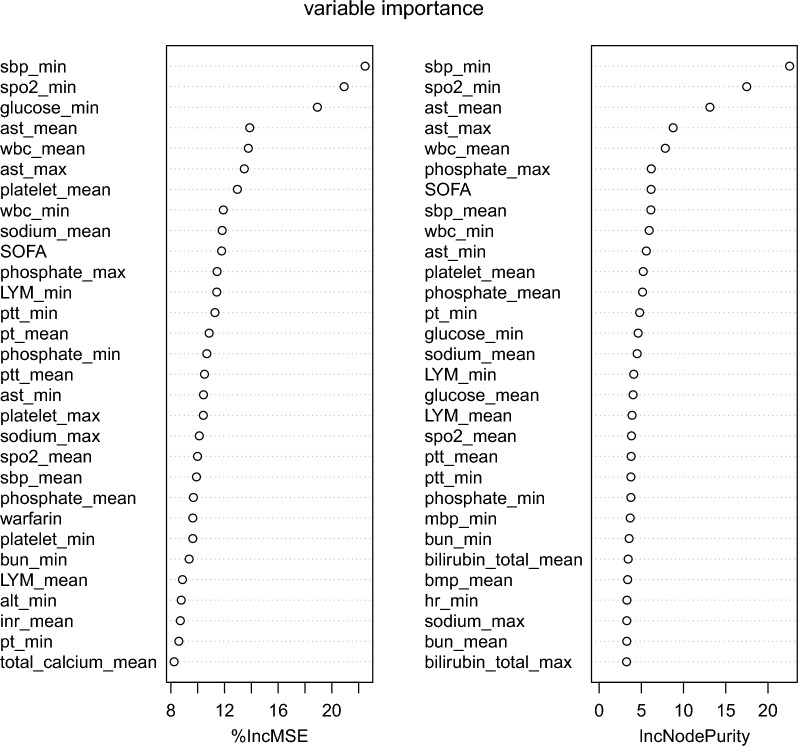
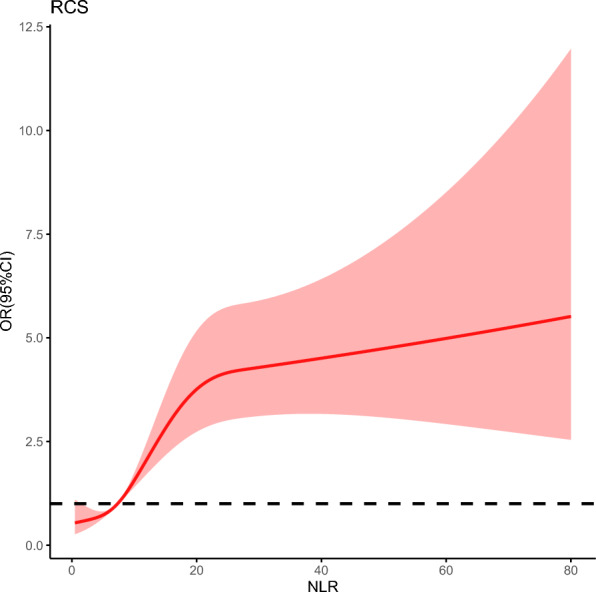
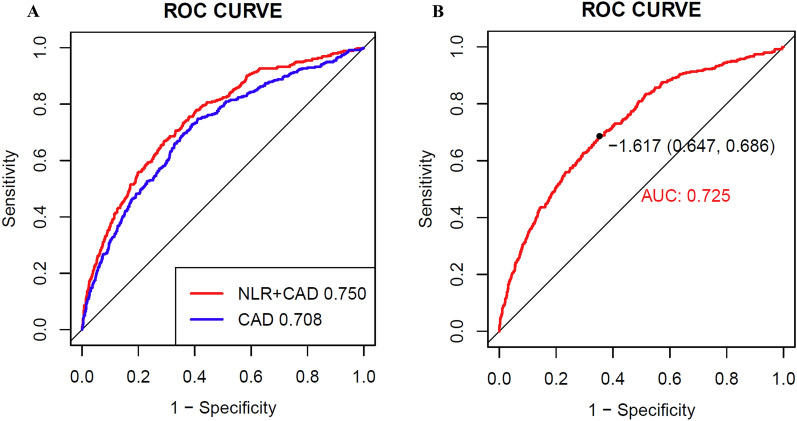
Methods: Data from the MIMIC-IV database, which includes a vast collection of more than 50,000 ICU admissions occurring between 2008 and 2019, was utilized in the study and eICU-CRD was conducted for external verification. The Boruta algorithm was employed for feature selection. Univariable and multivariable logistic regression analyses and multivariate restricted cubic spline regression were employed to scrutinize the association between NLR and in-hospital mortality. The receiver operating characteristic (ROC) curves were conducted to estimate the predictive ability of NLR.
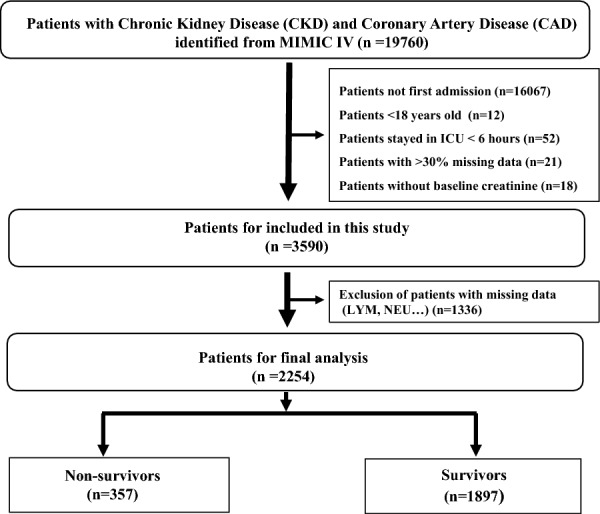
Results: After carefully applying criteria to include and exclude participants, a total of 2254 patients with CKD and CAD were included in the research. The findings showed a median NLR of 7.3 (4.4, 12.1). The outcomes of multivariable logistic regression demonstrated that NLR significantly elevated the risk of in-hospital mortality (OR 2.122, 95% confidence interval [CI] 1.542-2.921, P < 0.001) after accounting for all relevant factors. Further insights from subgroup analyses unveiled that age and Sequential Organ Failure Assessment (SOFA) scores displayed an interactive effect in the correlation between NLR and in-hospital deaths. The NLR combined with traditional cardiovascular risk factors showed relatively great predictive value for in-hospital mortality (AUC 0.750).
Conclusion: The findings of this research indicate that the NLR can be used as an indicator for predicting the likelihood of death during a patient's stay in the intensive care unit, particularly for individuals with both CAD and CKD. The results indicate that NLR may serve as a valuable tool for assessing and managing risks in this group at high risk. Further investigation is required to authenticate these findings and investigate the mechanisms that underlie the correlation between NLR and mortality in individuals with CAD and CKD.
Keywords: Chronic kidney disease; Coronary artery disease; In-hospital mortality; MIMIC-IV database; Neutrophil-to-lymphocyte ratio.
© 2024. The Author(s).
Conflict of interest statement
Not applicable.
Figures
Similar articles
-
Neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, platelet-to-lymphocyte ratio associated with 28-day all-cause mortality in septic patients with coronary artery disease: a retrospective analysis of MIMIC-IV database.BMC Infect Dis. 2024 Jul 29;24(1):749. doi: 10.1186/s12879-024-09516-5. BMC Infect Dis. 2024. PMID: 39075364 Free PMC article.
-
The neutrophil-to-lymphocyte ratio levels over time correlate to all-cause hospital mortality in sepsis.Heliyon. 2024 Aug 13;10(16):e36195. doi: 10.1016/j.heliyon.2024.e36195. eCollection 2024 Aug 30. Heliyon. 2024. PMID: 39253154 Free PMC article.
-
Association between the triglyceride glucose index and in-hospital and 1-year mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit.Cardiovasc Diabetol. 2023 May 13;22(1):110. doi: 10.1186/s12933-023-01843-2. Cardiovasc Diabetol. 2023. PMID: 37179310 Free PMC article.
-
The prognostic value of the combined neutrophil-to-lymphocyte ratio (NLR) and neutrophil-to-platelet ratio (NPR) in sepsis.Sci Rep. 2024 Jul 2;14(1):15075. doi: 10.1038/s41598-024-64469-8. Sci Rep. 2024. PMID: 38956445 Free PMC article.
-
The prediction of in-hospital mortality in chronic kidney disease patients with coronary artery disease using machine learning models.Eur J Med Res. 2023 Jan 18;28(1):33. doi: 10.1186/s40001-023-00995-x. Eur J Med Res. 2023. PMID: 36653875 Free PMC article.
Cited by
-
Neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, platelet-to-lymphocyte ratio associated with 28-day all-cause mortality in septic patients with coronary artery disease: a retrospective analysis of MIMIC-IV database.BMC Infect Dis. 2024 Jul 29;24(1):749. doi: 10.1186/s12879-024-09516-5. BMC Infect Dis. 2024. PMID: 39075364 Free PMC article.
References
-
- Gong P, Liu Y, Gong Y, Chen G, Zhang X, Wang S, et al. The association of neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and lymphocyte to monocyte ratio with post-thrombolysis early neurological outcomes in patients with acute ischemic stroke. J Neuroinflamm. 2021;18(1):51. doi: 10.1186/s12974-021-02090-6. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
