

Development of an adaptive clinical web-based prediction tool for kidney replacement therapy in children with chronic kidney disease
- PMID: 37391041
- PMCID: PMC10592093
- DOI: 10.1016/j.kint.2023.06.020
Development of an adaptive clinical web-based prediction tool for kidney replacement therapy in children with chronic kidney disease
Abstract
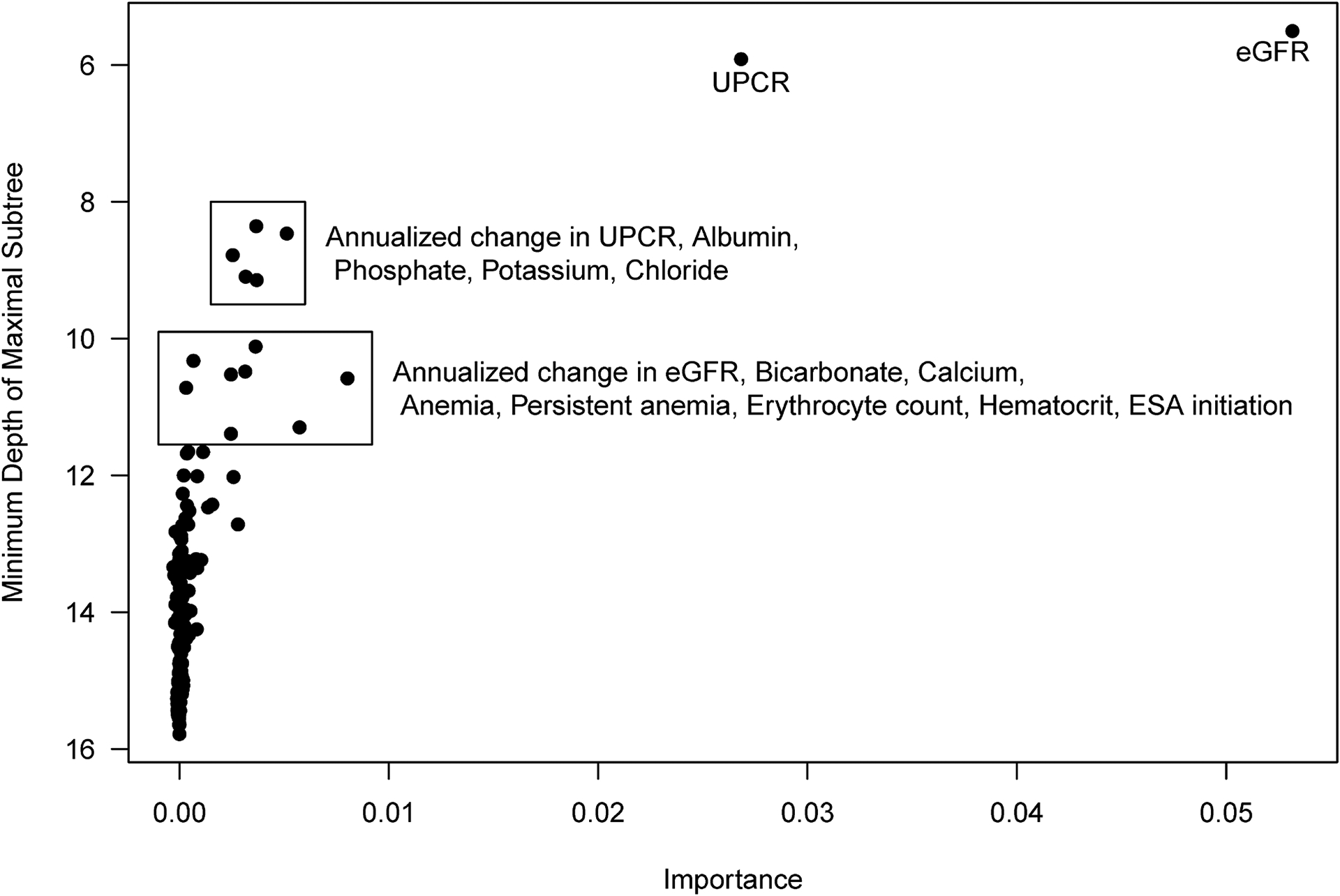
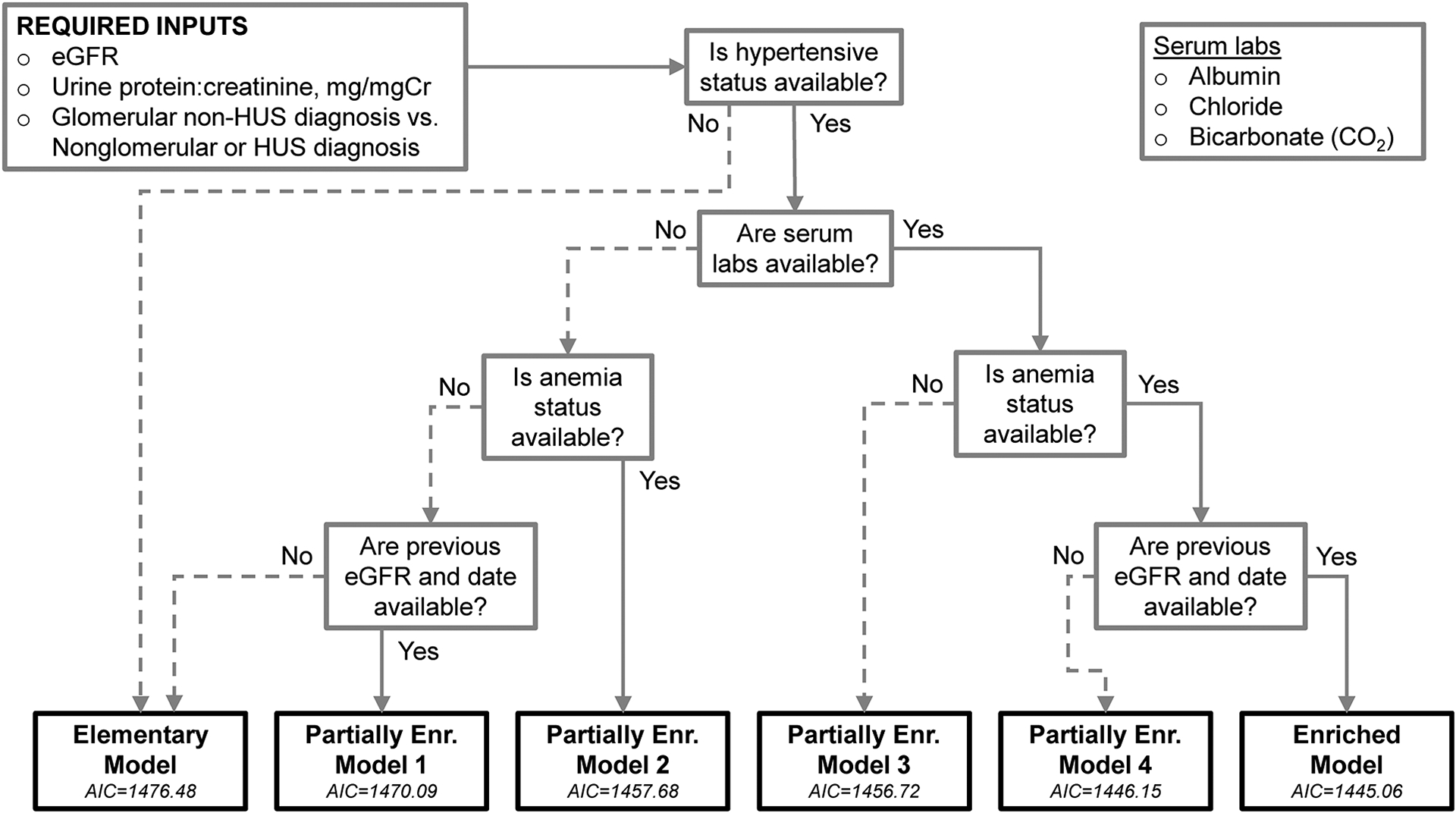
Clinicians need improved prediction models to estimate time to kidney replacement therapy (KRT) for children with chronic kidney disease (CKD). Here, we aimed to develop and validate a prediction tool based on common clinical variables for time to KRT in children using statistical learning methods and design a corresponding online calculator for clinical use. Among 890 children with CKD in the Chronic Kidney Disease in Children (CKiD) study, 172 variables related to sociodemographics, kidney/cardiovascular health, and therapy use, including longitudinal changes over one year were evaluated as candidate predictors in a random survival forest for time to KRT. An elementary model was specified with diagnosis, estimated glomerular filtration rate and proteinuria as predictors and then random survival forest identified nine additional candidate predictors for further evaluation. Best subset selection using these nine additional candidate predictors yielded an enriched model additionally based on blood pressure, change in estimated glomerular filtration rate over one year, anemia, albumin, chloride and bicarbonate. Four additional partially enriched models were constructed for clinical situations with incomplete data. Models performed well in cross-validation, and the elementary model was then externally validated using data from a European pediatric CKD cohort. A corresponding user-friendly online tool was developed for clinicians. Thus, our clinical prediction tool for time to KRT in children was developed in a large, representative pediatric CKD cohort with an exhaustive evaluation of potential predictors and supervised statistical learning methods. While our models performed well internally and externally, further external validation of enriched models is needed.
Keywords: kidney failure; kidney replacement therapy; pediatric chronic kidney disease; pediatric nephrology; prediction; risk stratification.
Copyright © 2023 International Society of Nephrology. All rights reserved.
Figures


Comment in
-
Predicting pediatric kidney disease progression-are 3 variables all you need?Kidney Int. 2023 Nov;104(5):885-887. doi: 10.1016/j.kint.2023.08.019. Kidney Int. 2023. PMID: 37863637
Similar articles
-
Predictors of Rapid Progression of Glomerular and Nonglomerular Kidney Disease in Children and Adolescents: The Chronic Kidney Disease in Children (CKiD) Cohort.Am J Kidney Dis. 2015 Jun;65(6):878-88. doi: 10.1053/j.ajkd.2015.01.008. Epub 2015 Mar 19. Am J Kidney Dis. 2015. PMID: 25799137 Free PMC article.
-
Association of Longitudinal B-Type Natriuretic Peptide Monitoring With Kidney Failure in Patients With CKD: A Cohort Study.Am J Kidney Dis. 2023 Nov;82(5):559-568. doi: 10.1053/j.ajkd.2023.05.003. Epub 2023 Jun 23. Am J Kidney Dis. 2023. PMID: 37354935
-
Estimating Time to ESRD in Children With CKD.Am J Kidney Dis. 2018 Jun;71(6):783-792. doi: 10.1053/j.ajkd.2017.12.011. Epub 2018 Apr 10. Am J Kidney Dis. 2018. PMID: 29653769 Free PMC article.
-
Kidney Disease Progression in Children and Young Adults With Pediatric CKD: Epidemiologic Perspectives and Clinical Applications.Semin Nephrol. 2021 Sep;41(5):405-415. doi: 10.1016/j.semnephrol.2021.09.002. Semin Nephrol. 2021. PMID: 34916001 Free PMC article. Review.
-
Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis.Health Technol Assess. 2010 Apr;14(21):1-184. doi: 10.3310/hta14210. Health Technol Assess. 2010. PMID: 20441712 Review.
References
-
- Peterson JC, Adler S, Burkart JM, et al. Blood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease Study. Ann Intern Med. 1995;123(10):754–762. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
