

Impact of Primary Tumor Location and Genomic Alterations on Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemoperfusion for Colorectal Peritoneal Metastases
- PMID: 37085655
- PMCID: PMC11225572
- DOI: 10.1245/s10434-023-13463-x
Impact of Primary Tumor Location and Genomic Alterations on Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemoperfusion for Colorectal Peritoneal Metastases
Abstract
Background: Colorectal cancer leads to peritoneal metastases (CRPM) in 10% of cases. Cytoreductive surgery with hyperthermic intraperitoneal chemoperfusion (CRS-HIPEC) improves survival. Primary tumor location and abnormalities in RAS, BRAF, and mismatch repair/microsatellite stability (MMR/MSI) may affect post-CRS-HIPEC survival, but studies have not been consistent. We estimated the effects of primary tumor site and genomic alterations on post-CRS-HIPEC survival.
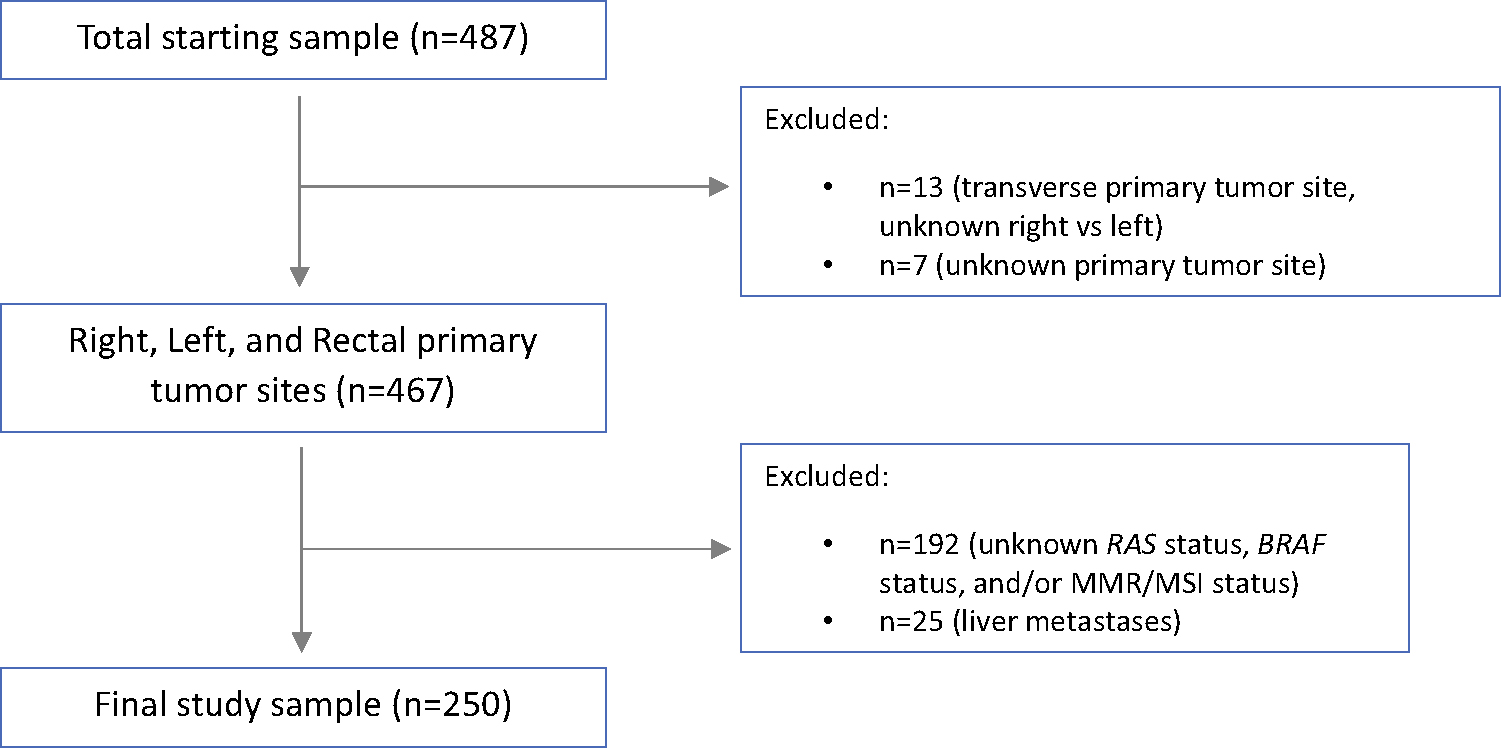
Methods: This retrospective cohort study included CRS-HIPEC cases for CRPM at a high-volume center from 2001 to 2020. Next-generation sequencing and microsatellite testing defined the RAS, BRAF, and MMR/MSI genotypes. Adjusted effects of tumor sidedness and genomics on survival were evaluated using a multivariable Cox proportional hazards model. We analyzed these variables' effects on progression-free survival and the effects of immune checkpoint-inhibitors.
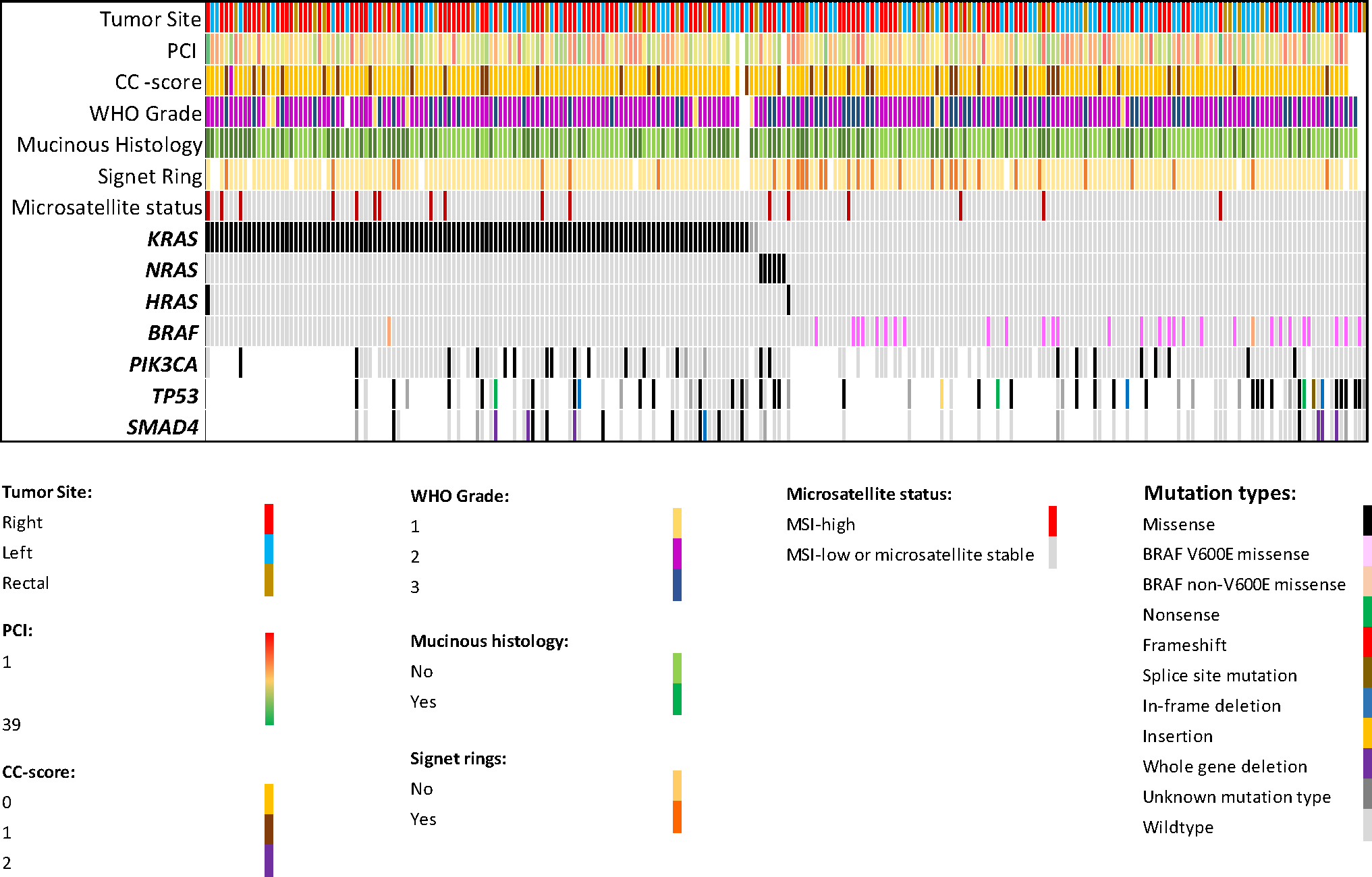
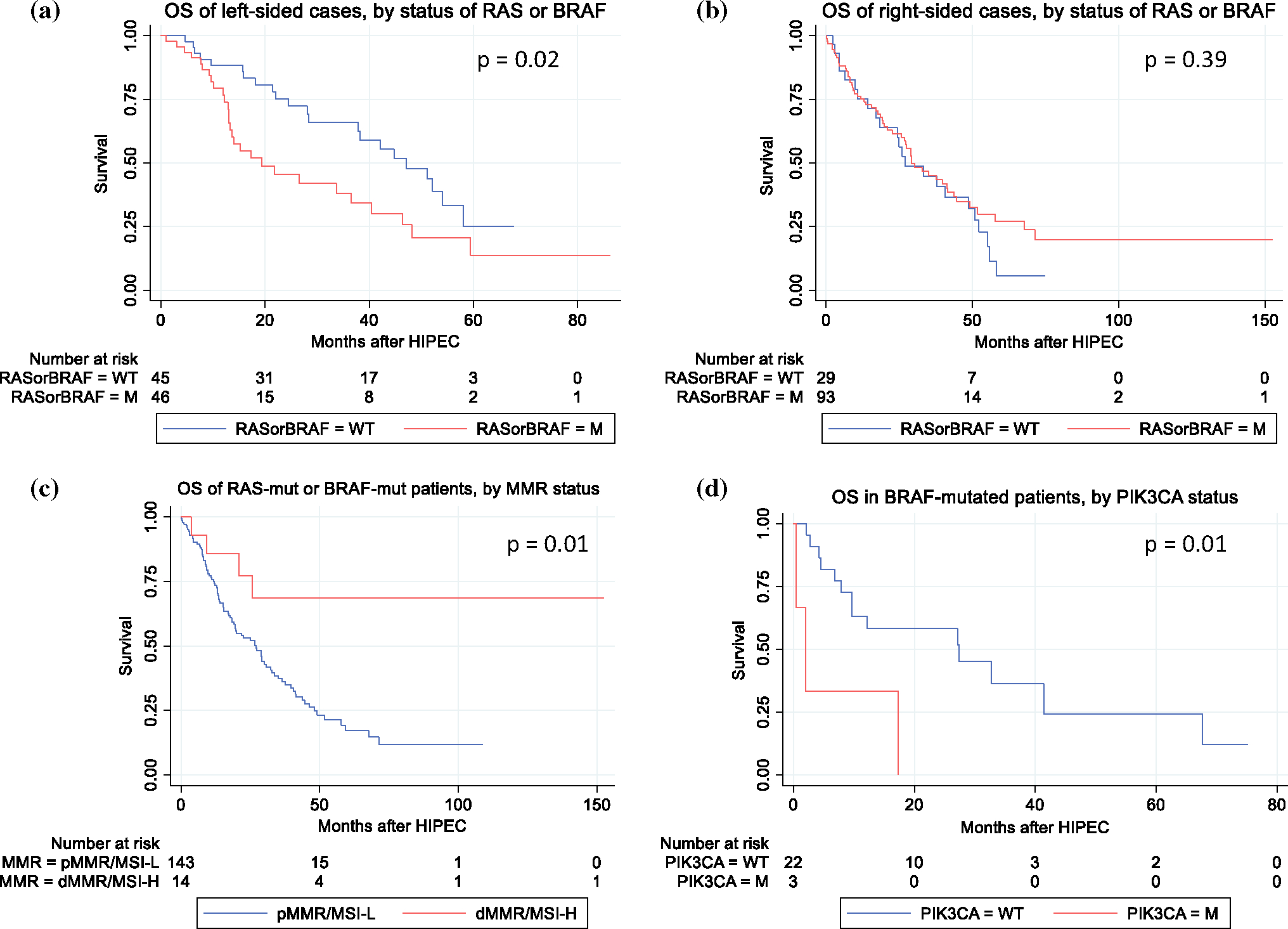
Results: A total of 250 patients underwent CRS-HIPEC with testing for RAS, BRAF, and MMR/MSI; 50.8% of patients were RAS-mutated, 12.4% were BRAF-mutated, and 6.8% were deficient-MMR/MSI-high (dMMR/MSI-H). Genomic alterations predominated in right-sided cancers. After adjustment for comorbidities and oncological and perioperative variables, rectal origin [hazard ratio (HR) 1.9, p = 0.01], RAS mutation (HR 1.6, p = 0.01), and BRAF mutation (HR 1.7, p = 0.05) were associated with worse survival. RAS mutation was also associated with shorter progression-free survival (HR 1.6, p = 0.01 at 6 months post-operatively), and dMMR/MSI-H status was associated with superior survival (HR 0.3, p = 0.01 at 2 years). dMMR/MSI-H patients receiving immune checkpoint-inhibitors trended toward superior survival.
Conclusions: Rectal origin, RAS mutations, and BRAF mutations are each associated with poorer survival after CRS-HIPEC for CRPM. Patients with CRPM and dMMR/MSI-H status have superior survival. Further research should evaluate benefits of immune checkpoint-inhibitors in this subgroup.
© 2023. Society of Surgical Oncology.
Figures
Comment in
-
ASO Author Reflections: Significance of Primary Tumor Location and Genomic Alterations in Colorectal Peritoneal Metastases and Cytoreductive Surgery-Hyperthermic Intraperitoneal Chemotherapy.Ann Surg Oncol. 2023 Jul;30(7):4471-4472. doi: 10.1245/s10434-023-13522-3. Epub 2023 Apr 27. Ann Surg Oncol. 2023. PMID: 37103724 Free PMC article. No abstract available.
Similar articles
-
Microsatellite and RAS/RAF Mutational Status as Prognostic Factors in Colorectal Peritoneal Metastases Treated with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC).Ann Surg Oncol. 2022 Jun;29(6):3405-3417. doi: 10.1245/s10434-021-11045-3. Epub 2021 Nov 16. Ann Surg Oncol. 2022. PMID: 34783946
-
The impact of molecular and mismatch repair status on the survival outcomes of surgically treated patients with colorectal peritoneal metastases.Eur J Surg Oncol. 2022 Oct;48(10):2218-2225. doi: 10.1016/j.ejso.2022.06.014. Epub 2022 Jun 18. Eur J Surg Oncol. 2022. PMID: 35750576
-
RAS Mutation Status Should Not Be Used to Predict Outcome from Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Colorectal Peritoneal Metastases.Ann Surg Oncol. 2023 Feb;30(2):792-801. doi: 10.1245/s10434-022-12704-9. Epub 2022 Nov 18. Ann Surg Oncol. 2023. PMID: 36400886 Free PMC article.
-
Prognostic factors influencing survival in patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy for isolated colorectal peritoneal metastases: a systematic review and meta-analysis.Colorectal Dis. 2020 Nov;22(11):1482-1495. doi: 10.1111/codi.15003. Epub 2020 Feb 27. Colorectal Dis. 2020. PMID: 32027455 Review.
-
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) for colorectal and appendiceal peritoneal metastases - The Hong Kong experience and literature review.Asian J Surg. 2021 Jan;44(1):221-228. doi: 10.1016/j.asjsur.2020.05.010. Epub 2020 Jun 27. Asian J Surg. 2021. PMID: 32605790 Review.
Cited by
-
ASO Author Reflections: Clinical Outcome After Upfront Curative-Intent Local Treatment of Metastases in Patient with Deficient Mismatch Repair Versus Proficient Mismatch Repair Metastatic Colorectal Cancer.Ann Surg Oncol. 2023 Oct;30(11):6771-6772. doi: 10.1245/s10434-023-14069-z. Epub 2023 Aug 10. Ann Surg Oncol. 2023. PMID: 37561342 Free PMC article. No abstract available.
-
Survival of Patients with Deficient Mismatch Repair Versus Proficient Mismatch Repair Metastatic Colorectal Cancer Receiving Curative-Intent Local Treatment of Metastases in a Nationwide Cohort.Ann Surg Oncol. 2023 Oct;30(11):6762-6770. doi: 10.1245/s10434-023-13974-7. Epub 2023 Aug 1. Ann Surg Oncol. 2023. PMID: 37528303 Free PMC article.
-
ASO Author Reflections: Significance of Primary Tumor Location and Genomic Alterations in Colorectal Peritoneal Metastases and Cytoreductive Surgery-Hyperthermic Intraperitoneal Chemotherapy.Ann Surg Oncol. 2023 Jul;30(7):4471-4472. doi: 10.1245/s10434-023-13522-3. Epub 2023 Apr 27. Ann Surg Oncol. 2023. PMID: 37103724 Free PMC article. No abstract available.
-
Survival Analysis and Recurrence Patterns in 555 Patients with Colorectal Peritoneal Metastases Treated by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy.Ann Surg Oncol. 2024 Dec;31(13):8585-8595. doi: 10.1245/s10434-024-15942-1. Epub 2024 Aug 11. Ann Surg Oncol. 2024. PMID: 39128977
-
Novel drug resistance mechanisms and drug targets in BRAF-mutated peritoneal metastasis from colorectal cancer.J Transl Med. 2024 Jul 9;22(1):646. doi: 10.1186/s12967-024-05467-2. J Transl Med. 2024. PMID: 38982444 Free PMC article.
References
-
- Franko J, Shi Q, Meyers JP, Maughan TS, Adams RA, Seymour MT, Saltz L, Punt CJA, Koopman M, Tournigand C, Tebbutt NC, Diaz-Rubio E, Souglakos J, et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomised trials from the analysis and research in cancers of the digestive system (ARCAD) database. Lancet Oncol. 2016;17(12):1709–19. - PubMed
-
- Quenet F, Elias D, Roca L, Goere D, Ghouti L, Pocard M, Facy O, Arvieux C, Lorimier G, Pezet D, Marchal F, Loi V, Meeus P, et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(2):256–66. - PubMed
-
- Verwaal VJ, van Ruth S, de Bree E, van Sloothen GW, van Tin-teren H, Boot H, Zoetmulder FA. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol. 2003;21(20):3737–43. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
