

Combinatorial biomarker for predicting outcomes to anti-PD-1 therapy in patients with metastatic clear cell renal cell carcinoma
- PMID: 36812889
- PMCID: PMC9975323
- DOI: 10.1016/j.xcrm.2023.100947
Combinatorial biomarker for predicting outcomes to anti-PD-1 therapy in patients with metastatic clear cell renal cell carcinoma
Abstract
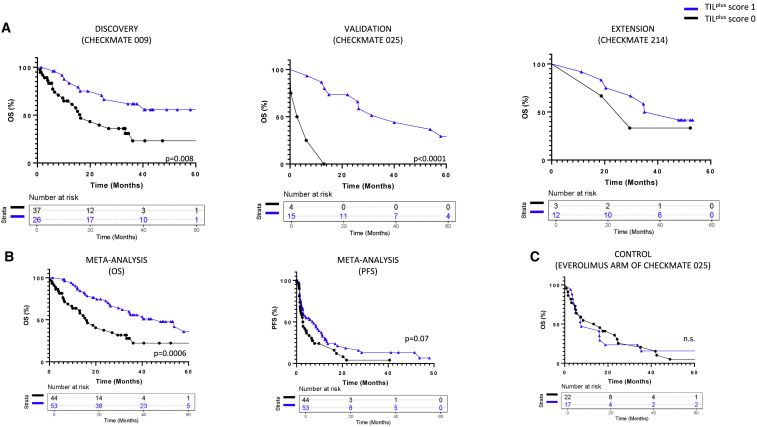
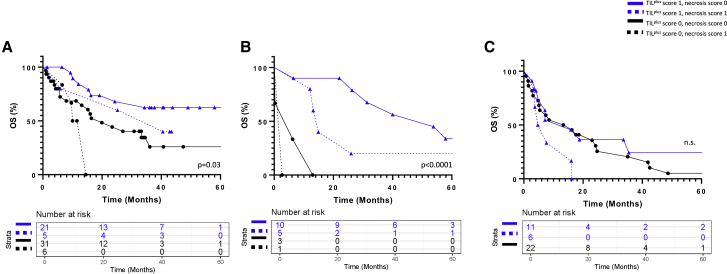
With a rapidly developing immunotherapeutic landscape for patients with metastatic clear cell renal cell carcinoma, biomarkers of efficacy are highly desirable to guide treatment strategy. Hematoxylin and eosin (H&E)-stained slides are inexpensive and widely available in pathology laboratories, including in resource-poor settings. Here, H&E scoring of tumor-infiltrating immune cells (TILplus) in pre-treatment tumor specimens using light microscopy is associated with improved overall survival (OS) in three independent cohorts of patients receiving immune checkpoint blockade. Necrosis score alone does not associate with OS; however, necrosis modifies the predictive effect of TILplus, a finding that has broad translational relevance for tissue-based biomarker development. PBRM1 mutational status is combined with H&E scores to further refine outcome predictions (OS, p = 0.007, and objective response, p = 0.04). These findings bring H&E assessment to the fore for biomarker development in future prospective, randomized trials, and emerging multi-omics classifiers.
Keywords: H&E; PBRM1; PD-1; RCC; TIL; biomarker; immunotherapy; irPRC; necrosis; pathologic response.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests Dr. Taube reports grants and consulting from Bristol-Myers Squibb and Akoya Biosciences, consulting for Merck, AstraZeneca, Genentech, GlaxoSmithKline, Regeneron, Lunaphore, and Compugen outside the submitted work. Dr. Deutsch and Dr. Taube report an institutional patent filed on machine learning for scoring pathologic response to immunotherapy. Dr. Topalian reports research grants from Bristol Myers Squibb; personal fees from AstraZeneca and Immunocore; and personal fees and stock options from Five Prime Therapeutics and Dragonfly Therapeutics. Dr. Topalian’s spouse has financial relationships with the following entities: Amgen, Bristol Myers Squibb, Compugen, DNAtrix, Dracen Pharmaceuticals, Enara Bio, Immunomic Therapeutics, Janssen Pharmaceuticals, ManaT Bio, RAPT Therapeutics, Tizona LLC, Trieza Therapeutics, TRex Bio Ltd, and WindMIL. Dr. Lipson receives institutional research grant funding from Bristol-Myers Squibb, Merck, and Regeneron, and during the past 2 years, has consulted for Bristol-Myers Squibb, Eisai, Genentech, Instil Bio, MacroGenics, Merck, Natera, Nektar Therapeutics, Odonate, OncoSec, Pfizer, Rain Therapeutics, Regeneron, and Sanofi Genzyme. Dr. Choueiri reports institutional and personal, paid and/or unpaid support for research, advisory boards, consultancy, and honoraria from AstraZeneca, Aravive, Aveo, Bayer, Bristol Myers-Squibb, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, IQVA, Infinity, Ipsen, Jansen, Kanaph, Lilly, Merck, Nikang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Surface Oncology, Takeda, Tempest, Up-To-Date, CME events (Peerview, OncLive, MJH, and others), outside the submitted work. Institutional patents filed on molecular alterations and immunotherapy response/toxicity, and ctDNA. Equity: Tempest, Pionyr, Osel, Precede Bio. CureResponse. Committees: NCCN, GU Steering Committee, ASCO/ESMO, ACCRU, KidneyCan. Medical writing and editorial assistance support may have been funded by Communications companies in part. No speaker’s bureau. Mentored several non-US citizens on research projects with potential funding (in part) from non-US sources/Foreign Components. The institution (Dana-Farber Cancer Institute) may have received additional independent funding of drug companies or/and royalties potentially involved in research around the subject matter. Dr. Atkins reports personal support for, advisory boards and consultancy from Bristol Myers Squibb, Merck, Eisai, Aveo, Pfizer, Werewolf, Fathom, Pyxis Oncology, PACT, Elpis, X4Pharma, ValoHealth, ScholarRock, Surface, Takeda, Simcha, Genentech-Roche, Exelixis, Iovance, COTA, Idera, Agenus, Asher Bio, Neoleukin, AstraZeneca, Calithera, SeaGen, Sanofi, SAB Bio, OncoRena, Pliant Therapeutics, Up-To-Date, and GlaxoSmithKline. Institutional Research support from BMS, Merck, and Pfizer and Stock or Stock options from Werewolf, Pyxis Oncology, and Elpis outside the submitted work. Dr. Signoretti reports receiving commercial research grants from Bristol-Myers Squibb, AstraZeneca, Exelixis, and Novartis; is a consultant/advisory board member for Merck, AstraZeneca, Bristol-Myers Squibb, CRISPR Therapeutics AG, AACR, and NCI; and receives royalties from Biogenex. Saurabh Gupta is a full-time employee of Bristol-Myers Squibb and owns BMS stock. Dr. Motzer reports clinical trial support (institutional) from BMS for this manuscript; advisory board fees from AstraZeneca, AVEO, Eisai, EMD Serono, Exelixis, Genentech/Roche, Incyte, Lilly Oncology, Merck, Novartis, and Pfizer; and fees (institutional) for coordinating PI from AVEO, BMS, Eisai, Exelixis, Genentech/Roche, Merck, and Pfizer. Dr. Ged reports advisory roles and has received honoraria from Aveo, Bristol Myers Squibb, BostonGene, and Exelixis. Drs. Baraban, Singla, Jedrych, and Danilova declare no competing interests.
Figures



Similar articles
-
Association of Machine Learning-Based Assessment of Tumor-Infiltrating Lymphocytes on Standard Histologic Images With Outcomes of Immunotherapy in Patients With NSCLC.JAMA Oncol. 2023 Jan 1;9(1):51-60. doi: 10.1001/jamaoncol.2022.4933. JAMA Oncol. 2023. PMID: 36394839 Free PMC article.
-
CTLA4 promoter hypomethylation is a negative prognostic biomarker at initial diagnosis but predicts response and favorable outcome to anti-PD-1 based immunotherapy in clear cell renal cell carcinoma.J Immunother Cancer. 2021 Aug;9(8):e002949. doi: 10.1136/jitc-2021-002949. J Immunother Cancer. 2021. PMID: 34446578 Free PMC article.
-
The Significance of PARP1 as a biomarker for Predicting the Response to PD-L1 Blockade in Patients with PBRM1-mutated Clear Cell Renal Cell Carcinoma.Eur Urol. 2022 Feb;81(2):145-148. doi: 10.1016/j.eururo.2021.09.024. Epub 2021 Oct 6. Eur Urol. 2022. PMID: 34627641
-
The journey of tumor-infiltrating lymphocytes as a biomarker in breast cancer: clinical utility in an era of checkpoint inhibition.Ann Oncol. 2021 Oct;32(10):1236-1244. doi: 10.1016/j.annonc.2021.07.007. Epub 2021 Jul 24. Ann Oncol. 2021. PMID: 34311075 Review.
-
Immune Checkpoint Inhibitors in the Treatment of Renal Cancer: Current State and Future Perspective.Int J Mol Sci. 2020 Jun 30;21(13):4691. doi: 10.3390/ijms21134691. Int J Mol Sci. 2020. PMID: 32630154 Free PMC article. Review.
Cited by
-
Exploring histological predictive biomarkers for immune checkpoint inhibitor therapy response in non-small cell lung cancer.J Pathol Transl Med. 2024 Mar;58(2):49-58. doi: 10.4132/jptm.2024.01.31. Epub 2024 Feb 26. J Pathol Transl Med. 2024. PMID: 38389279 Free PMC article. Review.
-
CXCL14 as a potential marker for immunotherapy response prediction in renal cell carcinoma.Ther Adv Med Oncol. 2023 Dec 25;15:17588359231217966. doi: 10.1177/17588359231217966. eCollection 2023. Ther Adv Med Oncol. 2023. PMID: 38152696 Free PMC article.
-
The 5th Kidney Cancer Research Summit: Research Accelerating Cures for Renal Cell Carcinoma in 2023.Oncologist. 2024 Feb 2;29(2):91-98. doi: 10.1093/oncolo/oyad322. Oncologist. 2024. PMID: 38048064 Free PMC article.
-
Association between pathologic response and survival after neoadjuvant therapy in lung cancer.Nat Med. 2024 Jan;30(1):218-228. doi: 10.1038/s41591-023-02660-6. Epub 2023 Oct 30. Nat Med. 2024. PMID: 37903504 Free PMC article.
-
Genomic Profiling and Molecular Characterization of Clear Cell Renal Cell Carcinoma.Curr Oncol. 2023 Oct 20;30(10):9276-9290. doi: 10.3390/curroncol30100670. Curr Oncol. 2023. PMID: 37887570 Free PMC article. Review.
References
-
- Rini B.I., Battle D., Figlin R.A., George D.J., Hammers H., Hutson T., Jonasch E., Joseph R.W., McDermott D.F., Motzer R.J., et al. The society for immunotherapy of cancer consensus statement on immunotherapy for the treatment of advanced renal cell carcinoma (RCC) J. Immunother. Cancer. 2019;7:354. - PMC - PubMed
-
- Reck M., Rodríguez-Abreu D., Robinson A.G., Hui R., Csőszi T., Fülöp A., Gottfried M., Peled N., Tafreshi A., Cuffe S., et al. Pembrolizumab versus chemotherapy for PD-L1–positive non–small-cell lung cancer. N. Engl. J. Med. 2016;375:1823–1833. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
