

Posttranslational modifications induce autoantibodies with risk prediction capability in patients with small cell lung cancer
- PMID: 36630482
- PMCID: PMC10117289
- DOI: 10.1126/scitranslmed.add8469
Posttranslational modifications induce autoantibodies with risk prediction capability in patients with small cell lung cancer
Abstract
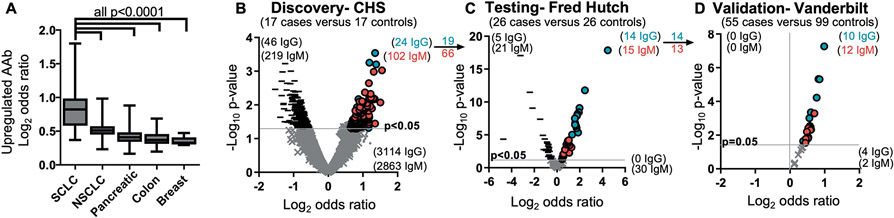
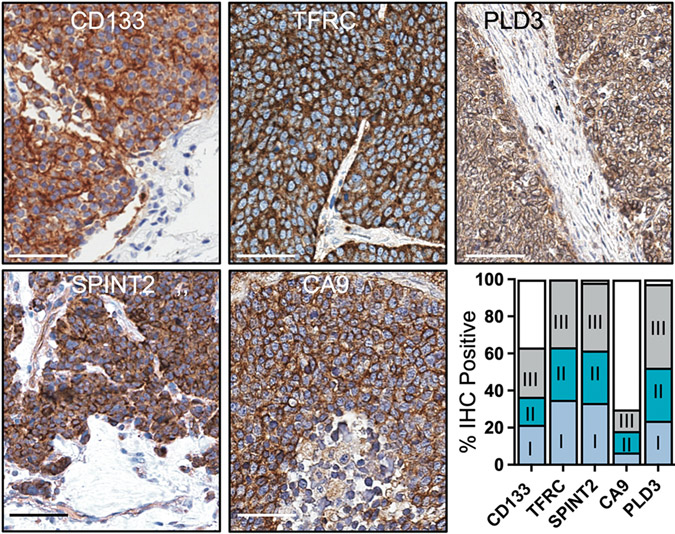
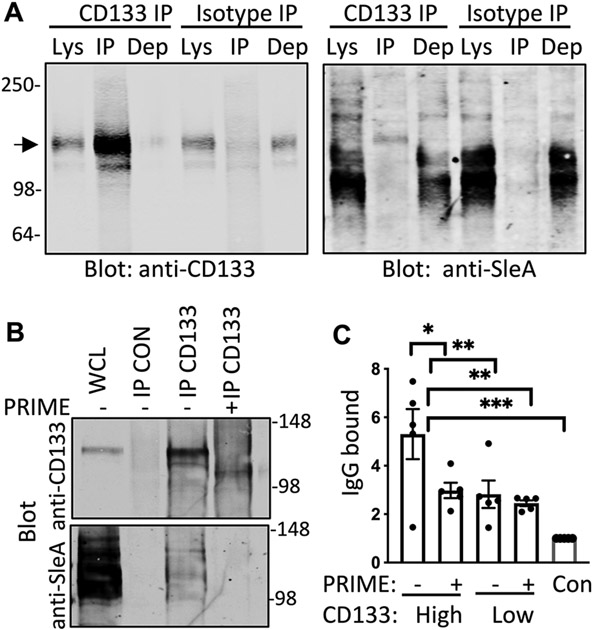
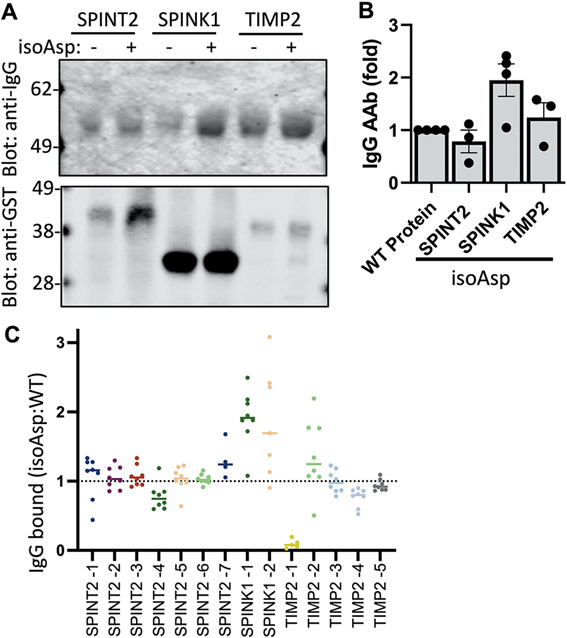
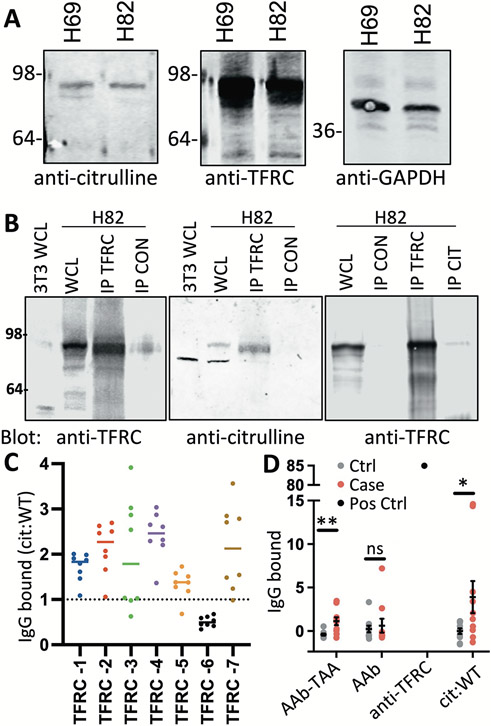
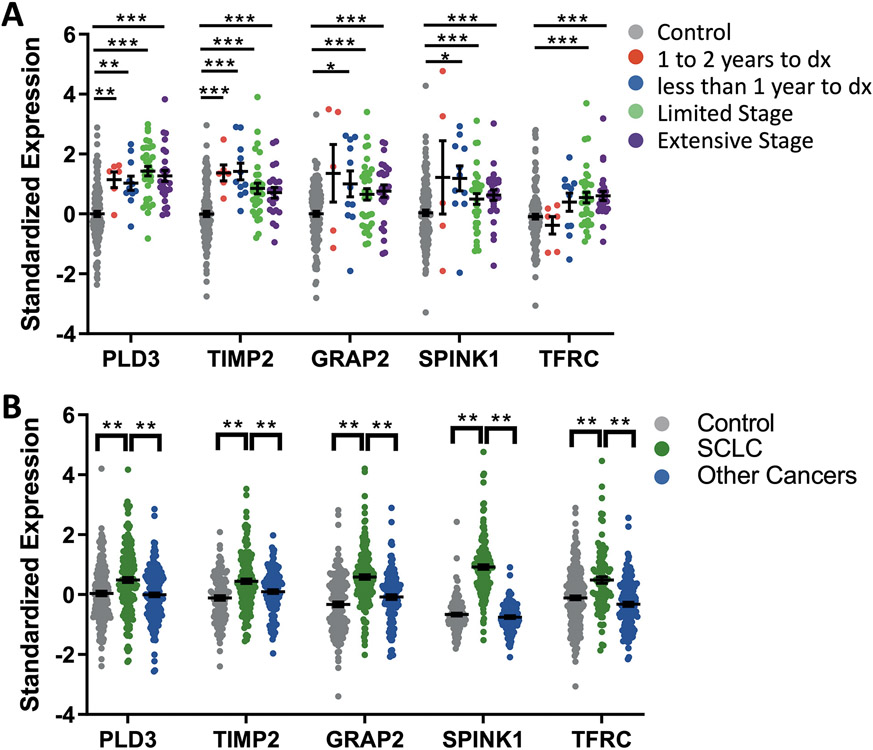
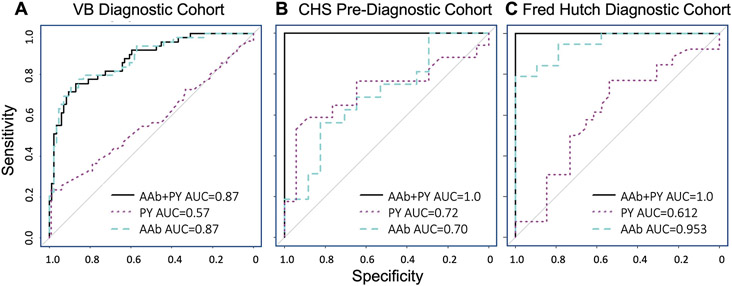
Small cell lung cancer (SCLC) elicits the generation of autoantibodies that result in unique paraneoplastic neurological syndromes. The mechanistic basis for the formation of such autoantibodies is largely unknown but is key to understanding their etiology. We developed a high-dimensional technique that enables detection of autoantibodies in complex with native antigens directly from patient plasma. Here, we used our platform to screen 1009 human plasma samples for 3600 autoantibody-antigen complexes, finding that plasma from patients with SCLC harbors, on average, fourfold higher disease-specific autoantibody signals compared with plasma from patients with other cancers. Across three independent SCLC cohorts, we identified a set of common but previously unknown autoantibodies that are produced in response to both intracellular and extracellular tumor antigens. We further characterized several disease-specific posttranslational modifications within extracellular proteins targeted by these autoantibodies, including citrullination, isoaspartylation, and cancer-specific glycosylation. Because most patients with SCLC have metastatic disease at diagnosis, we queried whether these autoantibodies could be used for SCLC early detection. We created a risk prediction model using five autoantibodies with an average area under the curve of 0.84 for the three cohorts that improved to 0.96 by incorporating cigarette smoke consumption in pack years. Together, our findings provide an innovative approach to identify circulating autoantibodies in SCLC with mechanistic insight into disease-specific immunogenicity and clinical utility.
Figures
Similar articles
-
Small-cell lung cancer-associated autoantibodies: potential applications to cancer diagnosis, early detection, and therapy.Mol Cancer. 2011 Mar 30;10:33. doi: 10.1186/1476-4598-10-33. Mol Cancer. 2011. PMID: 21450098 Free PMC article. Review.
-
Paraneoplastic autoimmunity and small-cell lung cancer: Neurological and serological accompaniments.Thorac Cancer. 2019 Apr;10(4):1001-1004. doi: 10.1111/1759-7714.13009. Epub 2019 Feb 27. Thorac Cancer. 2019. PMID: 30810271 Free PMC article.
-
An Autoantibody Subset Can Be Used for SCLC Early Detection.Cancer Discov. 2023 Mar 1;13(3):526. doi: 10.1158/2159-8290.CD-RW2023-009. Cancer Discov. 2023. PMID: 36661372
-
Paraneoplastic antigen Ma2 autoantibodies as specific blood biomarkers for detection of early recurrence of small intestine neuroendocrine tumors.PLoS One. 2010 Dec 30;5(12):e16010. doi: 10.1371/journal.pone.0016010. PLoS One. 2010. PMID: 21209860 Free PMC article.
-
[Paraneoplastic retinopathy and optic neuropathy].Brain Nerve. 2010 Apr;62(4):371-6. Brain Nerve. 2010. PMID: 20420177 Review. Japanese.
Cited by
-
Comparative Analysis of Antimicrobial Antibodies between Mild and Severe COVID-19.Microbiol Spectr. 2023 Aug 17;11(4):e0469022. doi: 10.1128/spectrum.04690-22. Epub 2023 Jun 6. Microbiol Spectr. 2023. PMID: 37278651 Free PMC article.
-
Breaking tolerance: autoantibodies can target protein posttranslational modifications.Curr Opin Biotechnol. 2024 Feb;85:103056. doi: 10.1016/j.copbio.2023.103056. Epub 2023 Dec 22. Curr Opin Biotechnol. 2024. PMID: 38141322 Review.
-
Glycosylation: mechanisms, biological functions and clinical implications.Signal Transduct Target Ther. 2024 Aug 5;9(1):194. doi: 10.1038/s41392-024-01886-1. Signal Transduct Target Ther. 2024. PMID: 39098853 Free PMC article. Review.
-
Autoantibody repertoire profiling in tissue and blood identifies colorectal cancer-specific biomarkers.Cancer Sci. 2024 Jan;115(1):83-93. doi: 10.1111/cas.16011. Epub 2023 Nov 20. Cancer Sci. 2024. PMID: 37985391 Free PMC article.
-
Multi-Omic Biomarkers Improve Indeterminate Pulmonary Nodule Malignancy Risk Assessment.Cancers (Basel). 2023 Jun 29;15(13):3418. doi: 10.3390/cancers15133418. Cancers (Basel). 2023. PMID: 37444527 Free PMC article.
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A, Cancer statistics, 2022. CA Cancer J Clin 72, 7–33 (2022). - PubMed
-
- Lindwasser OW, Ujhazy P, Antman MA, Prindiville SA, Small Cell Lung Cancer and the Recalcitrant Cancer Research Act. J Thorac Oncol 12, S1546 (2017).
Publication types
MeSH terms
Substances
Grants and funding
- U01 HL080295/HL/NHLBI NIH HHS/United States
- P30 CA015704/CA/NCI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01HC55222/HL/NHLBI NIH HHS/United States
- N01HC85086/HL/NHLBI NIH HHS/United States
- N01HC85083/HL/NHLBI NIH HHS/United States
- R01 CA243328/CA/NCI NIH HHS/United States
- N01HC85080/HL/NHLBI NIH HHS/United States
- P50 CA228944/CA/NCI NIH HHS/United States
- N01HC85081/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- U01 CA185097/CA/NCI NIH HHS/United States
- U01 CA152662/CA/NCI NIH HHS/United States
- U01 CA186157/CA/NCI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- N01HC85082/HL/NHLBI NIH HHS/United States
- KL2 TR002317/TR/NCATS NIH HHS/United States
- N01HC85079/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
