

Symptom burden and surgical outcome in non-skull base meningiomas
- PMID: 36212448
- PMCID: PMC9532974
- DOI: 10.3389/fonc.2022.967420
Symptom burden and surgical outcome in non-skull base meningiomas
Abstract
Purpose: Non-skull base meningiomas (NSBM) are a distinct entity and frequently present with focal neurological deficits. This study was designed to analyze functional and oncological outcome following microsurgical tumor resection in patients with NSBM.
Patients and methods: An analysis of 300 patients that underwent NSBM resection between 2003 and 2013 was performed. Assessment measures for functional outcome were Karnofsky Performance Scale (KPS), Medical Research Council - Neurological Performance Scale (MRC-NPS), and improvement rates of focal deficits and seizures. The extent of resection; recurrence-free survival (RFS) and tumor-specific survival (TSS) were also determined.
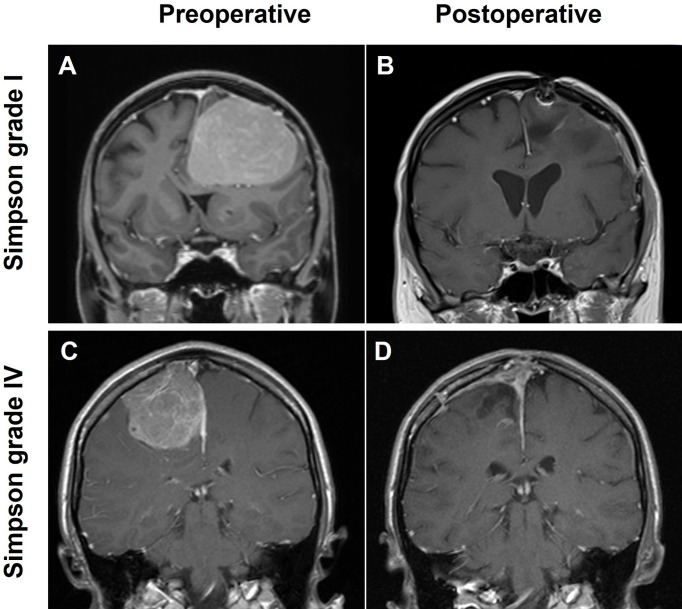
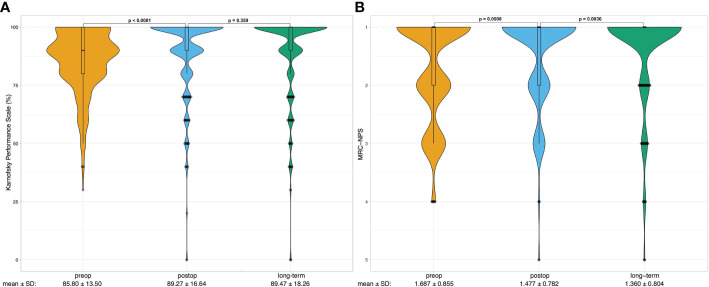
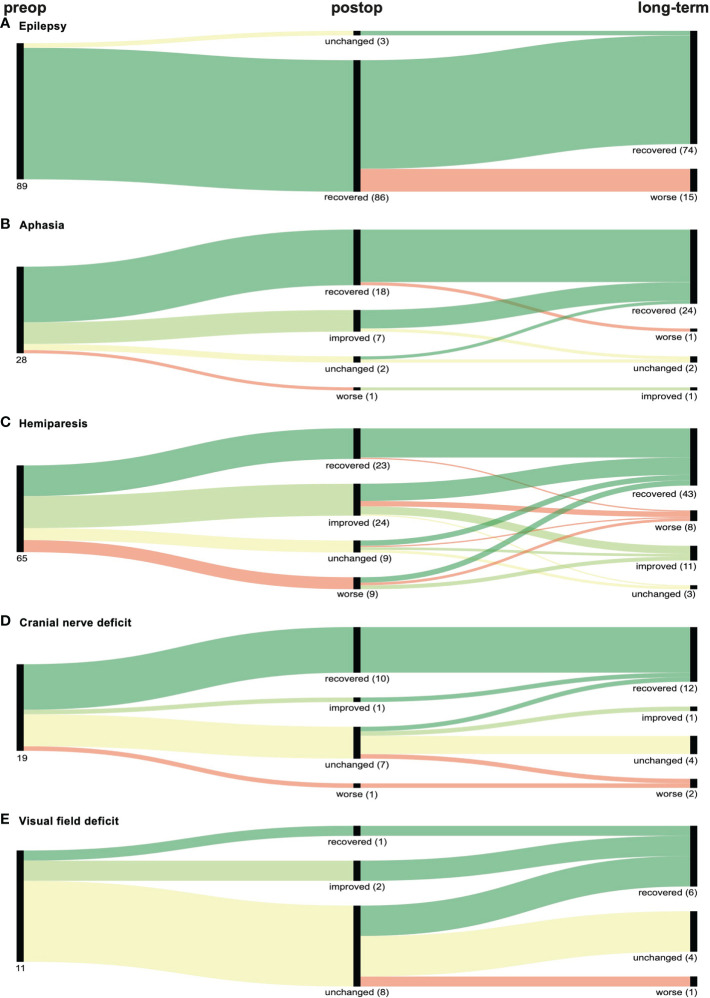
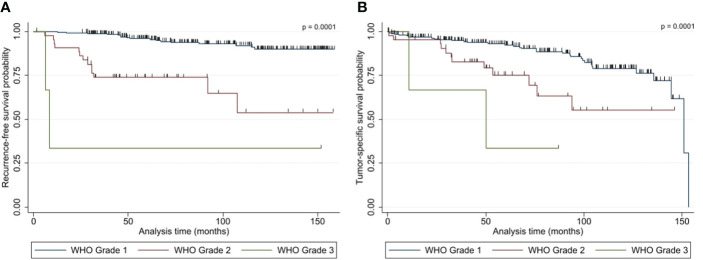
Results: Impaired KPS and MRC-NPS were present in 73.3% and 45.7%, respectively. Focal neurological deficits were recorded in 123 patients (41.0%), with hemiparesis (21.7%) and aphasia (9.3%) the most prevalent form of impairment. Most meningiomas were localized at the convexity (64.0%), followed by falcine tumors (20.3%). Both KPI and MRC-NPS scores were significantly improved by surgical resection. Postoperative improvement rates of 96.6%, 89.3%, 72.3%, 57.9%, and 27.3% were observed for aphasia, epilepsy, hemiparesis, cranial nerve, and visual field deficits, respectively. Long-term improvement was achieved in 83.2%, 89.3%, 80.0%, 68.4% and 54.6% of patients, respectively. Gross total resection (GTR) over subtotal resection (STR) significantly improved preoperative seizures and visual field deficits and correlated with reduced risk of new postoperative hemiparesis. Poor Simpson grade was the only significant prognostic factor in multivariate analysis for long-term functional deficit, which occurred in 7.3%. Median RFS was 45.9 months (6.0 - 151.5 months), while median TSS was 53.7 months (3.1 - 153.2 months). Both WHO grade (p= 0.001) and Simpson classification (p= 0.014 and p= 0.031) were independent significant prognostic factors for decreased RFS and TSS by multivariate analysis, respectively. Furthermore, tumor diameter > 50 mm (p= 0.039) significantly correlated with decreased TSS in multivariate analysis.
Conclusion: Surgical resection significantly and stably improves neurological deficits in patients with NSBM.
Keywords: meningioma; neurological deficit; outcome; recurrence; resection.
Copyright © 2022 Mederer, Schachinger, Rosengarth, Brosig, Schebesch, Doenitz, Schmidt and Proescholdt.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Skull base meningiomas: neurological outcome after microsurgical resection.J Neurooncol. 2014 Jan;116(2):381-6. doi: 10.1007/s11060-013-1309-x. Epub 2013 Nov 21. J Neurooncol. 2014. PMID: 24257965
-
True petroclival meningiomas: results of surgical management.J Neurosurg. 2014 Jan;120(1):40-51. doi: 10.3171/2013.8.JNS13535. Epub 2013 Oct 25. J Neurosurg. 2014. PMID: 24160473
-
Minimally invasive surgical treatment of intracranial meningiomas in elderly patients (≥ 65 years): outcomes, readmissions, and tumor control.Neurosurg Focus. 2020 Oct;49(4):E17. doi: 10.3171/2020.7.FOCUS20515. Neurosurg Focus. 2020. PMID: 33002879
-
Differential Tumor Progression Patterns in Skull Base Versus Non-Skull Base Meningiomas: A Critical Analysis from a Long-Term Follow-Up Study and Review of Literature.World Neurosurg. 2018 Apr;112:e74-e83. doi: 10.1016/j.wneu.2017.12.035. Epub 2017 Dec 16. World Neurosurg. 2018. PMID: 29258946 Review.
-
Surgical management of petroclival meningiomas: defining resection goals based on risk of neurological morbidity and tumor recurrence rates in 137 patients.Neurosurgery. 2005 Mar;56(3):546-59; discussion 546-59. doi: 10.1227/01.neu.0000153906.12640.62. Neurosurgery. 2005. PMID: 15730581 Review.
References
-
- DeMonte F, McDermott MW, Al-Mefty O. Al-Mefty´s meningiomas. 2nd ed. New York: Thieme Medical; (2011).
LinkOut - more resources
Full Text Sources