

Survival Benefit of First Single-Organ Deceased Donor Kidney Transplantation Compared With Long-term Dialysis Across Ages in Transplant-Eligible Patients With Kidney Failure
- PMID: 36205998
- PMCID: PMC9547326
- DOI: 10.1001/jamanetworkopen.2022.34971
Survival Benefit of First Single-Organ Deceased Donor Kidney Transplantation Compared With Long-term Dialysis Across Ages in Transplant-Eligible Patients With Kidney Failure
Abstract
Importance: Kidney transplant is considered beneficial in terms of survival compared with continued dialysis for patients with kidney failure. However, randomized clinical trials are infeasible, and available evidence from cohort studies is at high risk of bias.
Objective: To compare restricted mean survival times (RMSTs) between patients who underwent transplant and patients continuing dialysis across transplant candidate ages and depending on waiting time, applying target trial emulation methods.
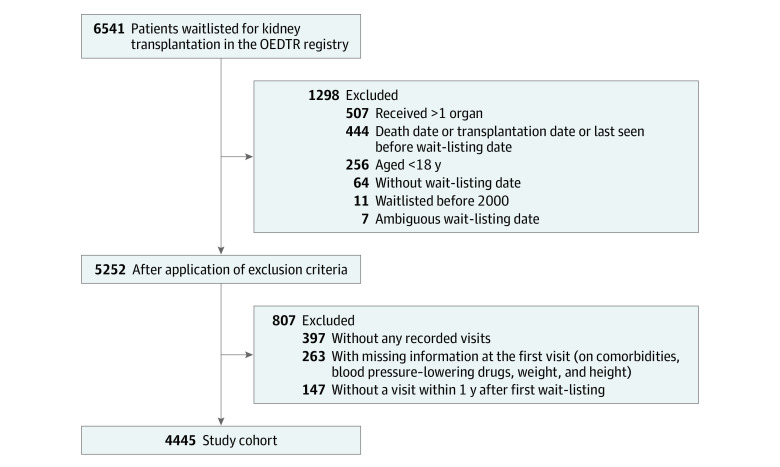
Design, setting, and participants: In this retrospective cohort study, patients aged 18 years or older appearing on the wait list for their first single-organ deceased donor kidney transplant between January 1, 2000, and December 31, 2018, in Austria were evaluated. Available data were obtained from the Austrian Dialysis and Transplant Registry and Eurotransplant and included repeated updates on wait-listing status and relevant covariates. Data were analyzed between August 1, 2019, and December 23, 2021.
Exposures: A target trial was emulated in which patients were randomized to either receive the transplant immediately (treatment group) or to continue dialysis and never receive a transplant (control group) at each time an organ became available.
Main outcomes and measures: The primary outcome was time from transplant allocation to death. Effect sizes in terms of RMSTs were obtained using a sequential Cox approach.
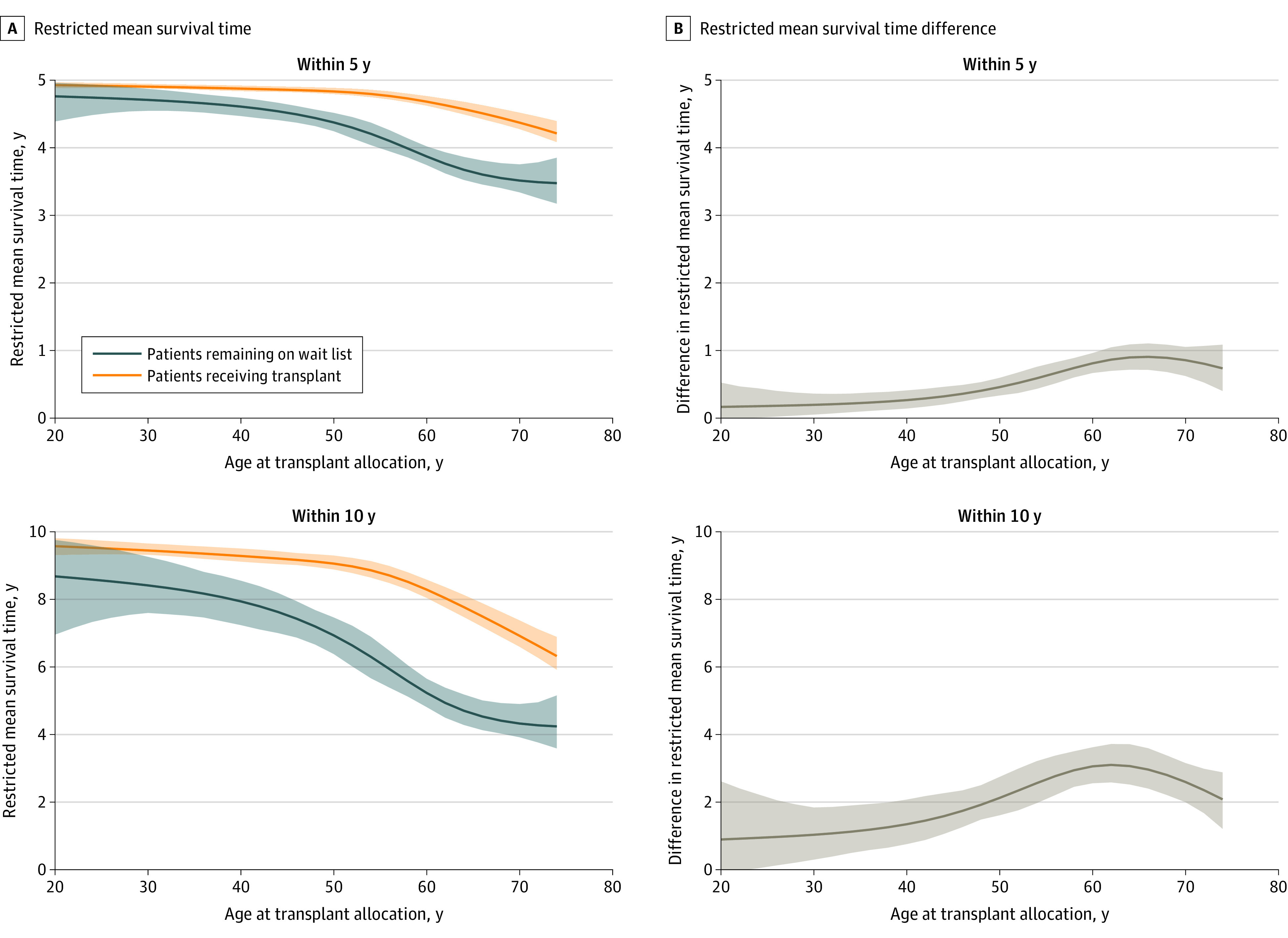
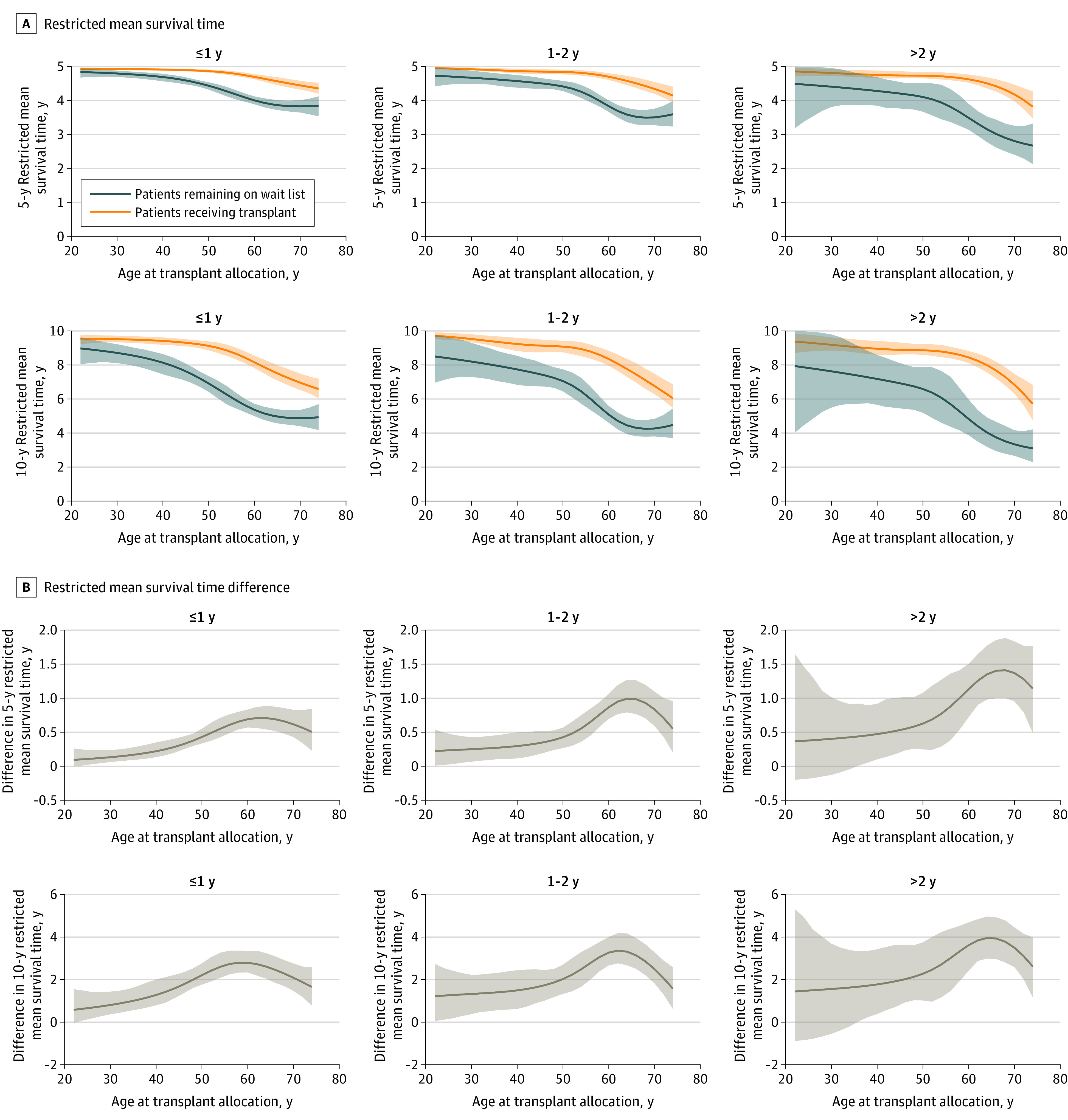
Results: Among the 4445 included patients (2974 men [66.9%]; mean [SD] age, 52.2 [13.2] years), transplant was associated with increased survival time across all considered ages compared with continuing dialysis and remaining on the wait list within a 10-year follow-up. The estimated RMST differences were 0.57 years (95% CI, -0.14 to 1.84 years) at age 20 years, 3.01 years (95% CI, 2.50 to 3.54 years) at age 60 years, and 2.48 years (95% CI, 1.88 to 3.04 years) at age 70 years. The survival benefit for patients who underwent transplant across ages was independent of waiting time.
Conclusions and relevance: The findings of this study suggest that kidney transplant prolongs the survival time of persons with kidney failure across all candidate ages and waiting times.
Conflict of interest statement
Figures
Similar articles
-
Association Between Declined Offers of Deceased Donor Kidney Allograft and Outcomes in Kidney Transplant Candidates.JAMA Netw Open. 2019 Aug 2;2(8):e1910312. doi: 10.1001/jamanetworkopen.2019.10312. JAMA Netw Open. 2019. PMID: 31469394 Free PMC article.
-
Association Between Dialysis Facility Ownership and Access to Kidney Transplantation.JAMA. 2019 Sep 10;322(10):957-973. doi: 10.1001/jama.2019.12803. JAMA. 2019. Retracted and republished in: JAMA. 2020 Apr 21;323(15):1509-1510. doi: 10.1001/jama.2020.2328. PMID: 31503308 Free PMC article. Retracted and republished.
-
Comparing the Net Benefits of Adult Deceased Donor Kidney Transplantation for a Patient on the Preemptive Waiting List vs a Patient Receiving Dialysis.JAMA Netw Open. 2022 Jul 1;5(7):e2223325. doi: 10.1001/jamanetworkopen.2022.23325. JAMA Netw Open. 2022. PMID: 35867058 Free PMC article.
-
The experiences of adults who are on dialysis and waiting for a renal transplant from a deceased donor: a systematic review.JBI Database System Rev Implement Rep. 2015 Mar 12;13(2):169-211. doi: 10.11124/jbisrir-2015-1973. JBI Database System Rev Implement Rep. 2015. PMID: 26447040 Review.
-
The UNOS Renal Transplant Registry: Review of the Last Decade.Clin Transpl. 2014:1-12. Clin Transpl. 2014. PMID: 26281122 Review.
Cited by
-
Twenty Years, and More to Come: Learning What Makes Some Transplants Ultra-Long Survivors.Transpl Int. 2022 Dec 5;35:11036. doi: 10.3389/ti.2022.11036. eCollection 2022. Transpl Int. 2022. PMID: 36545155 Free PMC article. No abstract available.
-
Reporting of Observational Studies Explicitly Aiming to Emulate Randomized Trials: A Systematic Review.JAMA Netw Open. 2023 Sep 5;6(9):e2336023. doi: 10.1001/jamanetworkopen.2023.36023. JAMA Netw Open. 2023. PMID: 37755828 Free PMC article.
-
Effect of post-transplant diabetes mellitus on cardiovascular events and mortality: a single-center retrospective cohort study.Endocrine. 2024 Aug;85(2):695-703. doi: 10.1007/s12020-024-03770-y. Epub 2024 Mar 15. Endocrine. 2024. PMID: 38491339
-
Comorbid Conditions in Kidney Transplantation: Outcome Analysis at King Abdulaziz Medical City.Cureus. 2023 Jul 4;15(7):e41355. doi: 10.7759/cureus.41355. eCollection 2023 Jul. Cureus. 2023. PMID: 37546132 Free PMC article.
-
Sex differences in the survival benefit of kidney transplantation: a retrospective cohort study using target trial emulation.Nephrol Dial Transplant. 2023 Dec 20;39(1):36-44. doi: 10.1093/ndt/gfad137. Nephrol Dial Transplant. 2023. PMID: 37403325 Free PMC article.
References
-
- Jensen CE, Sørensen P, Petersen KD. In Denmark kidney transplantation is more cost-effective than dialysis. Dan Med J. 2014;61(3):A4796. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
