

Physical Exercise Modalities for the Management of Heart Failure With Preserved Ejection Fraction: A Systematic Review and Meta-Analysis
- PMID: 35522702
- PMCID: PMC9067087
- DOI: 10.1097/FJC.0000000000001254
Physical Exercise Modalities for the Management of Heart Failure With Preserved Ejection Fraction: A Systematic Review and Meta-Analysis
Abstract
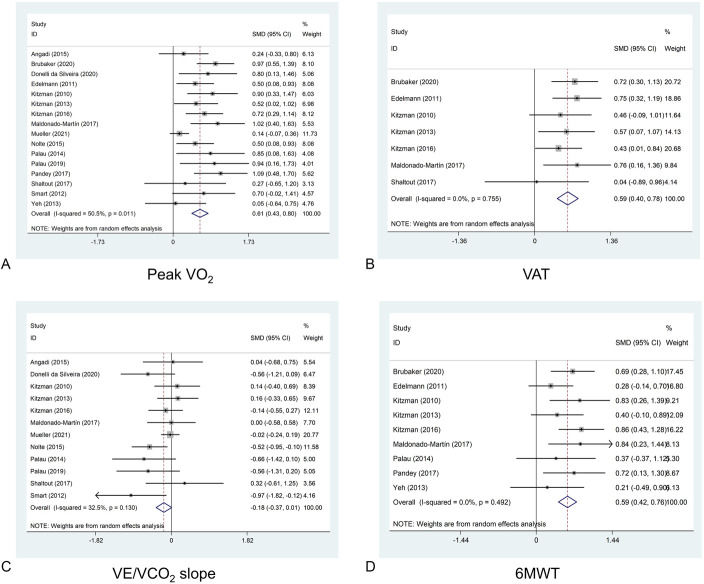
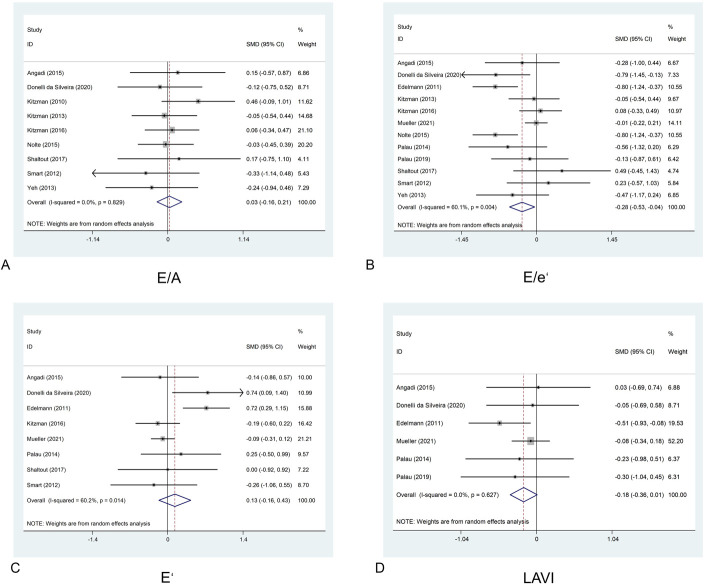
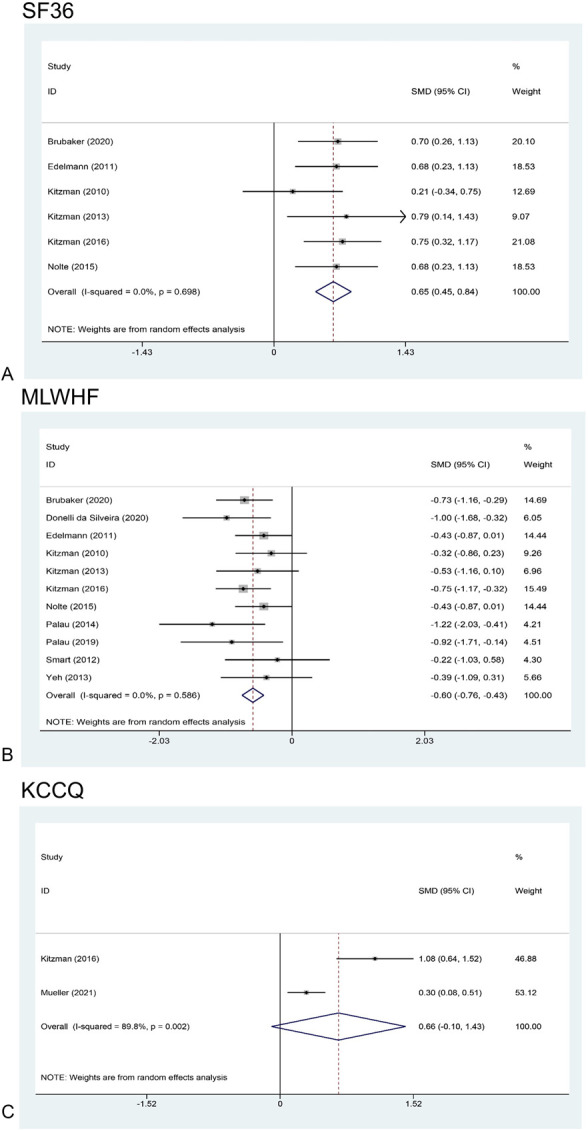
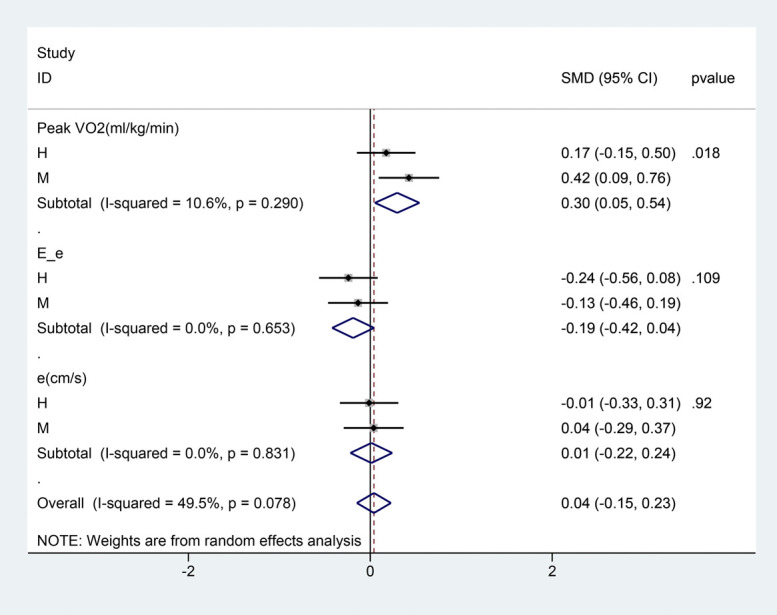
Different physical exercise modalities have been widely studied in patients having heart failure with preserved ejection fraction (HFpEF) but with variably reported findings. We, therefore, conducted a systematic review and meta-analysis to evaluate whether the efficacy of physical activity in the management of HFpEF is related to exercise modalities. PubMed and Embase were searched up to July 2021. The eligible studies included randomized controlled trials that identified effects of physical exercise on patients with HFpEF. Sixteen studies were included to evaluate the efficiency of physical exercise in HFpEF. A pooled analysis showed that exercise training significantly improved peak oxygen uptake (VO2), ventilatory anaerobic threshold, distance covered in the 6-minute walking test, the ratio of early diastolic mitral inflow to annular velocities, the Short Form 36 physical component score, and the Minnesota Living with Heart Failure Questionnaire total score. However, the changes in other echocardiographic parameters including the ratio of peak early to late diastolic mitral inflow velocities, early diastolic mitral annular velocity, and left atrial volume index were not significant. Both high-intensity and moderate-intensity training significantly improved exercise capacity (as defined by peak VO2), with moderate-intensity exercise having a superior effect. Furthermore, exercise-induced improvement in peak VO2 was partially correlated with exercise duration. Physical exercise could substantially improve exercise capacity, quality of life, and some indicators of cardiac diastolic function in patients with HFpEF. A protocol of moderate-intensity exercise training lasting a longer duration might be more beneficial compared with high-intensity training for patients with HFpEF.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Does Intensity Really Matter to Improve Cardiorespiratory Fitness in Patients With Heart Failure With Preserved Ejection Fraction?J Cardiovasc Pharmacol. 2022 Oct 1;80(4):493-495. doi: 10.1097/FJC.0000000000001323. J Cardiovasc Pharmacol. 2022. PMID: 35905475 No abstract available.
Similar articles
-
Phosphodiesterase inhibitor for heart failure with preserved ejection fraction: A systematic review and meta-analysis.Saudi Pharm J. 2022 Aug;30(8):1079-1087. doi: 10.1016/j.jsps.2022.05.012. Epub 2022 Jun 1. Saudi Pharm J. 2022. PMID: 36164567 Free PMC article.
-
Effects of exercise training on cardiac function, exercise capacity, and quality of life in heart failure with preserved ejection fraction: a meta-analysis of randomized controlled trials.Heart Fail Rev. 2019 Jul;24(4):535-547. doi: 10.1007/s10741-019-09774-5. Heart Fail Rev. 2019. PMID: 31032533
-
Effects of mineralocorticoid receptor antagonists on left ventricular diastolic function, exercise capacity, and quality of life in heart failure with preserved ejection fraction: a meta-analysis of randomized controlled trials.Heart Vessels. 2019 Apr;34(4):597-606. doi: 10.1007/s00380-018-1279-1. Epub 2018 Oct 12. Heart Vessels. 2019. PMID: 30315496 Review.
-
Functional iron deficiency and diastolic function in heart failure with preserved ejection fraction.Int J Cardiol. 2013 Oct 12;168(5):4652-7. doi: 10.1016/j.ijcard.2013.07.185. Epub 2013 Jul 30. Int J Cardiol. 2013. PMID: 23968714
-
Exercise training in patients with heart failure and preserved ejection fraction: meta-analysis of randomized control trials.Circ Heart Fail. 2015 Jan;8(1):33-40. doi: 10.1161/CIRCHEARTFAILURE.114.001615. Epub 2014 Nov 16. Circ Heart Fail. 2015. PMID: 25399909 Free PMC article. Review.
Cited by
-
Impact of Exercise Training at Different Intensity Levels on Cardiac Function and Exercise Capacity in Patients with Chronic Heart Failure: A Prospective Cohort Study.J Rehabil Med. 2022 Nov 4;54:jrm00347. doi: 10.2340/jrm.v54.1023. J Rehabil Med. 2022. PMID: 36264054 Free PMC article.
-
Lifestyle interventions in cardiometabolic HFpEF: dietary and exercise modalities.Heart Fail Rev. 2024 Sep 16. doi: 10.1007/s10741-024-10439-1. Online ahead of print. Heart Fail Rev. 2024. PMID: 39283525 Review.
-
Phosphodiesterase inhibitor for heart failure with preserved ejection fraction: A systematic review and meta-analysis.Saudi Pharm J. 2022 Aug;30(8):1079-1087. doi: 10.1016/j.jsps.2022.05.012. Epub 2022 Jun 1. Saudi Pharm J. 2022. PMID: 36164567 Free PMC article.
-
Diagnostic and therapeutic challenges for PCPs regarding heart failure with preserved ejection fraction and obesity: results of an online internet-based survey.BMC Prim Care. 2024 Aug 8;25(1):288. doi: 10.1186/s12875-024-02549-4. BMC Prim Care. 2024. PMID: 39118004 Free PMC article.
-
Exercise training improves exercise capacity and quality of life in heart failure with preserved ejection fraction: a systematic review and meta-analysis of randomized controlled trials.Eur Heart J Open. 2024 Jun 26;4(4):oeae033. doi: 10.1093/ehjopen/oeae033. eCollection 2024 Jul. Eur Heart J Open. 2024. PMID: 38982996 Free PMC article.
References
-
- Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2017;14:591–602. - PubMed
-
- Bozkurt B, Fonarow GC, Goldberg LR, et al. Cardiac rehabilitation for patients with heart failure: JACC Expert Panel. J Am Coll Cardiol. 2021;77:1454–1469. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
