

Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer
- PMID: 35403841
- PMCID: PMC9844511
- DOI: 10.1056/NEJMoa2202170
Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer
Abstract
Background: Neoadjuvant or adjuvant chemotherapy confers a modest benefit over surgery alone for resectable non-small-cell lung cancer (NSCLC). In early-phase trials, nivolumab-based neoadjuvant regimens have shown promising clinical activity; however, data from phase 3 trials are needed to confirm these findings.
Methods: In this open-label, phase 3 trial, we randomly assigned patients with stage IB to IIIA resectable NSCLC to receive nivolumab plus platinum-based chemotherapy or platinum-based chemotherapy alone, followed by resection. The primary end points were event-free survival and pathological complete response (0% viable tumor in resected lung and lymph nodes), both evaluated by blinded independent review. Overall survival was a key secondary end point. Safety was assessed in all treated patients.
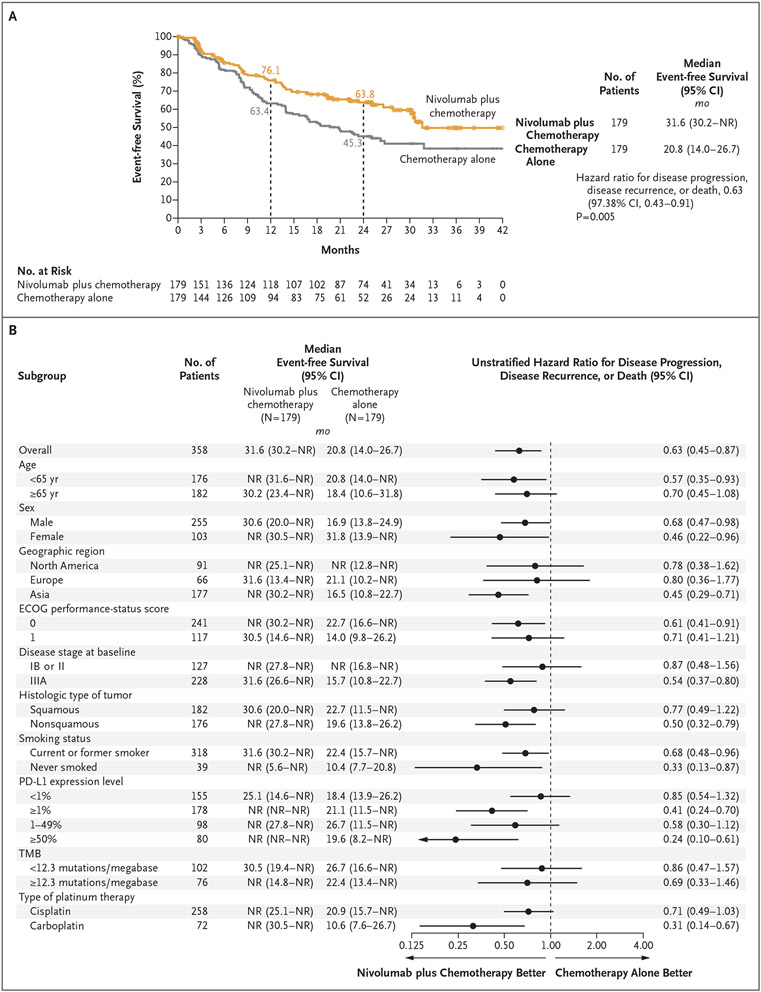
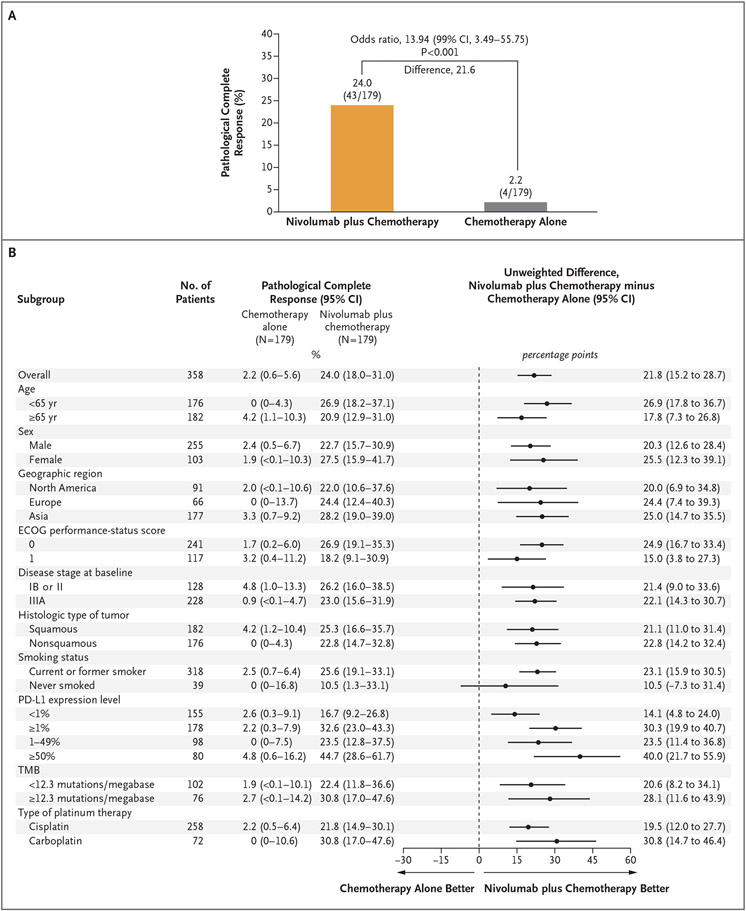
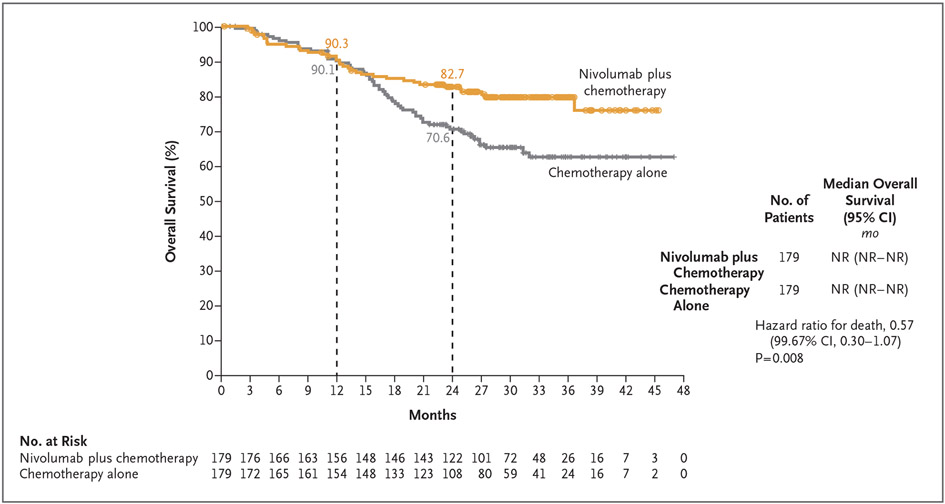
Results: The median event-free survival was 31.6 months (95% confidence interval [CI], 30.2 to not reached) with nivolumab plus chemotherapy and 20.8 months (95% CI, 14.0 to 26.7) with chemotherapy alone (hazard ratio for disease progression, disease recurrence, or death, 0.63; 97.38% CI, 0.43 to 0.91; P = 0.005). The percentage of patients with a pathological complete response was 24.0% (95% CI, 18.0 to 31.0) and 2.2% (95% CI, 0.6 to 5.6), respectively (odds ratio, 13.94; 99% CI, 3.49 to 55.75; P<0.001). Results for event-free survival and pathological complete response across most subgroups favored nivolumab plus chemotherapy over chemotherapy alone. At the first prespecified interim analysis, the hazard ratio for death was 0.57 (99.67% CI, 0.30 to 1.07) and did not meet the criterion for significance. Of the patients who underwent randomization, 83.2% of those in the nivolumab-plus-chemotherapy group and 75.4% of those in the chemotherapy-alone group underwent surgery. Grade 3 or 4 treatment-related adverse events occurred in 33.5% of the patients in the nivolumab-plus-chemotherapy group and in 36.9% of those in the chemotherapy-alone group.
Conclusions: In patients with resectable NSCLC, neoadjuvant nivolumab plus chemotherapy resulted in significantly longer event-free survival and a higher percentage of patients with a pathological complete response than chemotherapy alone. The addition of nivolumab to neoadjuvant chemotherapy did not increase the incidence of adverse events or impede the feasibility of surgery. (Funded by Bristol Myers Squibb; CheckMate 816 ClinicalTrials.gov number, NCT02998528.).
Copyright © 2022 Massachusetts Medical Society.
Figures
Comment in
-
Expanding Horizons for Treatment of Early-Stage Lung Cancer.N Engl J Med. 2022 May 26;386(21):2050-2051. doi: 10.1056/NEJMe2203330. Epub 2022 Apr 11. N Engl J Med. 2022. PMID: 35403840 No abstract available.
-
Role of neoadjuvant chemoimmunotherapy for resectable NSCLC.Nat Rev Clin Oncol. 2022 Aug;19(8):497-498. doi: 10.1038/s41571-022-00647-9. Nat Rev Clin Oncol. 2022. PMID: 35585121 No abstract available.
-
When immunotherapy meets surgery in non-small cell lung cancer.Cancer Cell. 2022 Jun 13;40(6):603-605. doi: 10.1016/j.ccell.2022.05.010. Epub 2022 Jun 2. Cancer Cell. 2022. PMID: 35660136
-
Neoadjuvant therapy gains FDA approval in non-small cell lung cancer.Cell Rep Med. 2022 Jul 19;3(7):100691. doi: 10.1016/j.xcrm.2022.100691. Cell Rep Med. 2022. PMID: 35858590 Free PMC article. Clinical Trial.
-
Neoadjuvant Nivolumab plus Chemotherapy in Lung Cancer.N Engl J Med. 2022 Aug 11;387(6):571. doi: 10.1056/NEJMc2208133. N Engl J Med. 2022. PMID: 35947717 No abstract available.
-
Neoadjuvant Nivolumab plus Chemotherapy in Lung Cancer.N Engl J Med. 2022 Aug 11;387(6):571-572. doi: 10.1056/NEJMc2208133. N Engl J Med. 2022. PMID: 35947718 No abstract available.
Similar articles
-
Perioperative Nivolumab and Chemotherapy in Stage III Non-Small-Cell Lung Cancer.N Engl J Med. 2023 Aug 10;389(6):504-513. doi: 10.1056/NEJMoa2215530. Epub 2023 Jun 28. N Engl J Med. 2023. PMID: 37379158 Clinical Trial.
-
Perioperative Nivolumab in Resectable Lung Cancer.N Engl J Med. 2024 May 16;390(19):1756-1769. doi: 10.1056/NEJMoa2311926. N Engl J Med. 2024. PMID: 38749033 Clinical Trial.
-
Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer.N Engl J Med. 2019 Nov 21;381(21):2020-2031. doi: 10.1056/NEJMoa1910231. Epub 2019 Sep 28. N Engl J Med. 2019. PMID: 31562796 Clinical Trial.
-
Preoperative chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual participant data.Lancet. 2014 May 3;383(9928):1561-71. doi: 10.1016/S0140-6736(13)62159-5. Epub 2014 Feb 25. Lancet. 2014. PMID: 24576776 Free PMC article. Review.
-
Comparative Efficacy and Safety of Neoadjuvant Immunotherapy with Nivolumab vs. Pembrolizumab in Resectable Non-Small Cell Lung Cancer: A Systematic Review.Curr Oncol. 2024 Oct 18;31(10):6289-6299. doi: 10.3390/curroncol31100469. Curr Oncol. 2024. PMID: 39451773 Free PMC article. Review.
Cited by
-
Heterogeneity in peripheral blood immune lymphocyte subsets predicts the response of immunotherapy or chemoradiotherapy in advanced lung cancer: an analysis across different pathological types, treatment modalities and age.Front Immunol. 2024 Oct 17;15:1464728. doi: 10.3389/fimmu.2024.1464728. eCollection 2024. Front Immunol. 2024. PMID: 39483483 Free PMC article.
-
The role of PD-L1 in patients with non-small cell lung cancer receiving neoadjuvant immune checkpoint inhibitor plus chemotherapy: a meta-analysis.Sci Rep. 2024 Oct 31;14(1):26200. doi: 10.1038/s41598-024-78159-y. Sci Rep. 2024. PMID: 39482343 Free PMC article.
-
Perioperative sintilimab and neoadjuvant anlotinib plus chemotherapy for resectable non-small-cell lung cancer: a multicentre, open-label, single-arm, phase 2 trial (TD-NeoFOUR trial).Signal Transduct Target Ther. 2024 Oct 28;9(1):296. doi: 10.1038/s41392-024-01992-0. Signal Transduct Target Ther. 2024. PMID: 39465257 Free PMC article. Clinical Trial.
-
Evidence for the evolving role of neoadjuvant and perioperative immunotherapy in resectable non-small cell lung cancer.Explor Target Antitumor Ther. 2024;5(6):1247-1260. doi: 10.37349/etat.2024.00273. Epub 2024 Sep 29. Explor Target Antitumor Ther. 2024. PMID: 39465010 Free PMC article. Review.
-
Immunotherapy response induces divergent tertiary lymphoid structure morphologies in hepatocellular carcinoma.Nat Immunol. 2024 Nov;25(11):2110-2123. doi: 10.1038/s41590-024-01992-w. Epub 2024 Oct 25. Nat Immunol. 2024. PMID: 39455893
References
-
- Taylor MD, Nagji AS, Bhamidipati CM, et al. Tumor recurrence after complete resection for non-small cell lung cancer. Ann Thorac Surg 2012;93:1813–20. - PubMed
-
- National Comprehensive Cancer Network. Guidelines for treatment of cancer by type: non-small cell lung cancer. Version 2.2022. 2022.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical