

Population Immunity and Covid-19 Severity with Omicron Variant in South Africa
- PMID: 35196424
- PMCID: PMC8908853
- DOI: 10.1056/NEJMoa2119658
Population Immunity and Covid-19 Severity with Omicron Variant in South Africa
Abstract
Background: The B.1.1.529 (omicron) variant of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified on November 25, 2021, in Gauteng province, South Africa. Data regarding the seroprevalence of SARS-CoV-2 IgG in Gauteng before the fourth wave of coronavirus disease 2019 (Covid-19), in which the omicron variant was dominant, are needed.
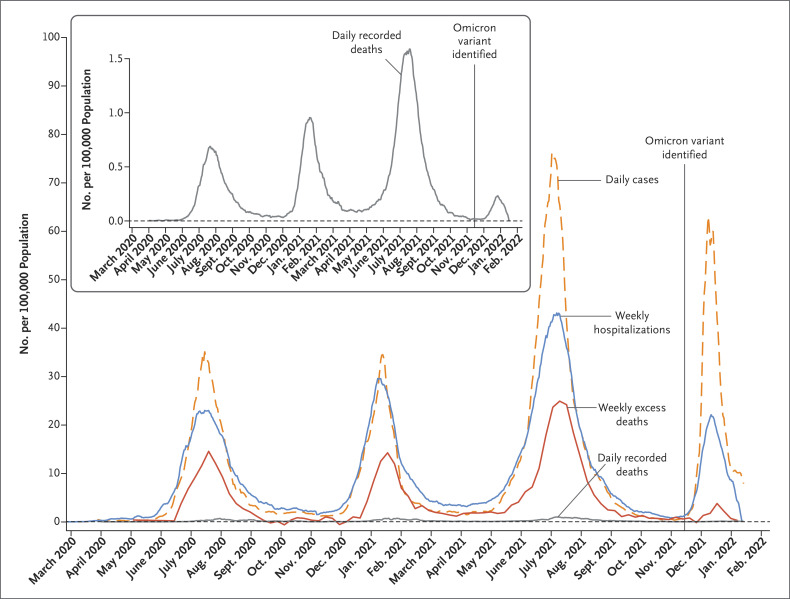
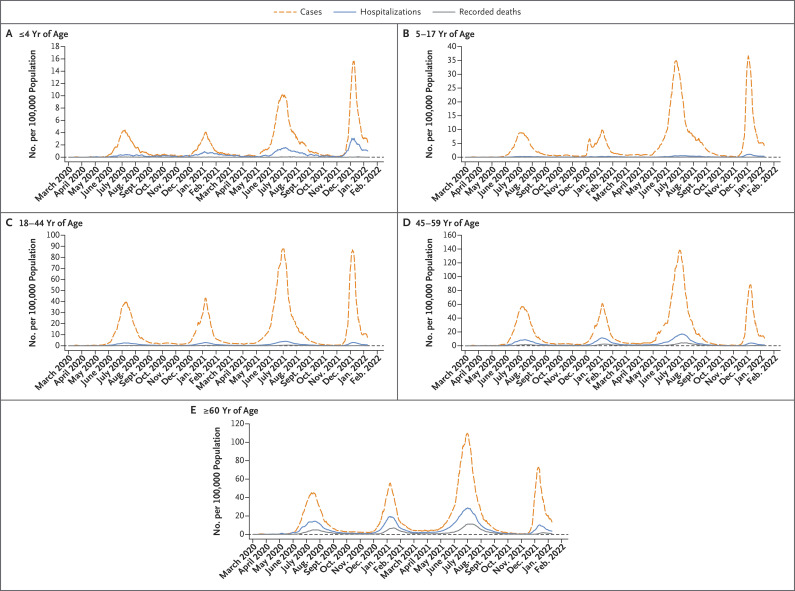
Methods: We conducted a seroepidemiologic survey from October 22 to December 9, 2021, in Gauteng to determine the seroprevalence of SARS-CoV-2 IgG. Households included in a previous seroepidemiologic survey (conducted from November 2020 to January 2021) were contacted; to account for changes in the survey population, there was a 10% increase in the households contacted, with the use of the same sampling framework. Dried-blood-spot samples were tested for IgG against SARS-CoV-2 spike protein and nucleocapsid protein with the use of quantitative assays. We also evaluated Covid-19 epidemiologic trends in Gauteng, including cases, hospitalizations, recorded deaths, and excess deaths from the start of the pandemic through January 12, 2022.
Results: Samples were obtained from 7010 participants, of whom 1319 (18.8%) had received a Covid-19 vaccine. The seroprevalence of SARS-CoV-2 IgG ranged from 56.2% (95% confidence interval [CI], 52.6 to 59.7) among children younger than 12 years of age to 79.7% (95% CI, 77.6 to 81.5) among adults older than 50 years of age. Vaccinated participants were more likely to be seropositive for SARS-CoV-2 than unvaccinated participants (93.1% vs. 68.4%). Epidemiologic data showed that the incidence of SARS-CoV-2 infection increased and subsequently declined more rapidly during the fourth wave than it had during the three previous waves. The incidence of infection was decoupled from the incidences of hospitalization, recorded death, and excess death during the fourth wave, as compared with the proportions seen during previous waves.
Conclusions: Widespread underlying SARS-CoV-2 seropositivity was observed in Gauteng before the omicron-dominant wave of Covid-19. Epidemiologic data showed a decoupling of hospitalizations and deaths from infections while omicron was circulating. (Funded by the Bill and Melinda Gates Foundation.).
Copyright © 2022 Massachusetts Medical Society.
Figures

Similar articles
-
Omicron B.1.1.529 variant infections associated with severe disease are uncommon in a COVID-19 under-vaccinated, high SARS-CoV-2 seroprevalence population in Malawi.EClinicalMedicine. 2023 Feb;56:101800. doi: 10.1016/j.eclinm.2022.101800. Epub 2022 Dec 30. EClinicalMedicine. 2023. PMID: 36600885 Free PMC article.
-
SARS-CoV-2 infection and mortality during the first epidemic wave in Madurai, south India: a prospective, active surveillance study.Lancet Infect Dis. 2021 Dec;21(12):1665-1676. doi: 10.1016/S1473-3099(21)00393-5. Epub 2021 Aug 13. Lancet Infect Dis. 2021. PMID: 34399090 Free PMC article.
-
Safety and immunogenicity of a modified mRNA-lipid nanoparticle vaccine candidate against COVID-19: Results from a phase 1, dose-escalation study.Hum Vaccin Immunother. 2024 Dec 31;20(1):2408863. doi: 10.1080/21645515.2024.2408863. Epub 2024 Oct 18. Hum Vaccin Immunother. 2024. PMID: 39422261 Free PMC article. Clinical Trial.
-
Topical fluoride as a cause of dental fluorosis in children.Cochrane Database Syst Rev. 2024 Jun 20;6(6):CD007693. doi: 10.1002/14651858.CD007693.pub3. Cochrane Database Syst Rev. 2024. PMID: 38899538 Review.
-
Interventions for supporting pregnant women's decision-making about mode of birth after a caesarean.Cochrane Database Syst Rev. 2013 Jul 30;2013(7):CD010041. doi: 10.1002/14651858.CD010041.pub2. Cochrane Database Syst Rev. 2013. PMID: 23897547 Free PMC article. Review.
Cited by
-
Clinical usefulness of testing for severe acute respiratory syndrome coronavirus 2 antibodies.Eur J Intern Med. 2023 Jan;107:7-16. doi: 10.1016/j.ejim.2022.11.009. Epub 2022 Nov 10. Eur J Intern Med. 2023. PMID: 36379820 Free PMC article. Review.
-
Estimation of vaccine effectiveness against SARS-CoV-2-associated hospitalization using sentinel surveillance in South Africa.Int J Epidemiol. 2024 Aug 14;53(5):dyae116. doi: 10.1093/ije/dyae116. Int J Epidemiol. 2024. PMID: 39305220 Free PMC article.
-
SARS-CoV-2 Variants Infection in Relationship to Imaging-based Pneumonia and Clinical Outcomes.Radiology. 2023 Mar;306(3):e221795. doi: 10.1148/radiol.221795. Epub 2022 Sep 27. Radiology. 2023. PMID: 36165791 Free PMC article.
-
SARS-CoV-2 Omicron BA.1 and BA.2 are attenuated in rhesus macaques as compared to Delta.Sci Adv. 2022 Nov 16;8(46):eade1860. doi: 10.1126/sciadv.ade1860. Epub 2022 Nov 18. Sci Adv. 2022. PMID: 36399566 Free PMC article.
-
The Risk Factors and Outcomes for Radiological Abnormalities in Early Convalescence of COVID-19 Patients Caused by the SARS-CoV-2 Omicron Variant: A Retrospective, Multicenter Follow-up Study.J Korean Med Sci. 2023 Feb 27;38(8):e55. doi: 10.3346/jkms.2023.38.e55. J Korean Med Sci. 2023. PMID: 36852851 Free PMC article.
References
-
- Callaway E. Heavily mutated Omicron variant puts scientists on alert. Nature 2021;600:21-21. - PubMed
-
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 variant of concern. November 26, 2021. (https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1....).
-
- European Centre for Disease Prevention and Control. Implications of the emergence and spread of the SARS-CoV-2 B.1.1. 529 variant of concern (Omicron) for the EU/EEA. November 26, 2021. (https://www.ecdc.europa.eu/sites/default/files/documents/Implications-em...).
-
- UK Health Security Agency. SARS-CoV-2 variants of concern and variants under investigation in England: technical briefing 29. November 26, 2021. (https://assets.publishing.service.gov.uk/government/uploads/system/uploa...).
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous