

Increased Platelet-CD4+ T Cell Aggregates Are Correlated With HIV-1 Permissiveness and CD4+ T Cell Loss
- PMID: 34987521
- PMCID: PMC8720770
- DOI: 10.3389/fimmu.2021.799124
Increased Platelet-CD4+ T Cell Aggregates Are Correlated With HIV-1 Permissiveness and CD4+ T Cell Loss
Abstract
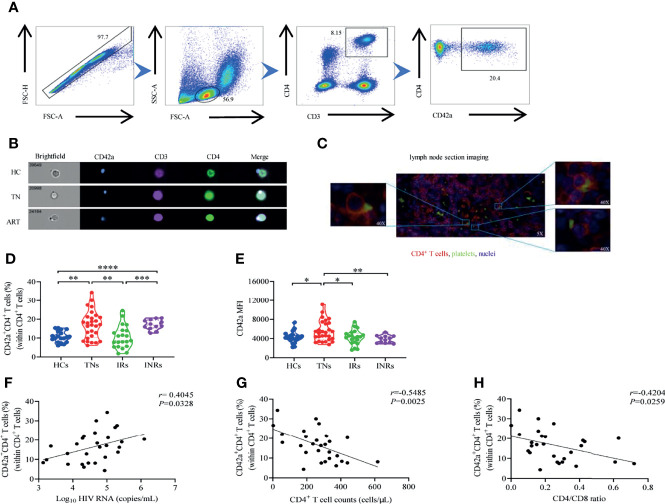
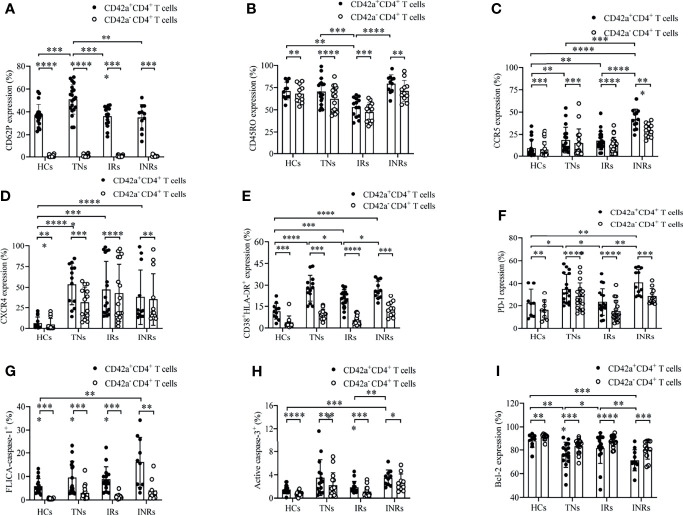
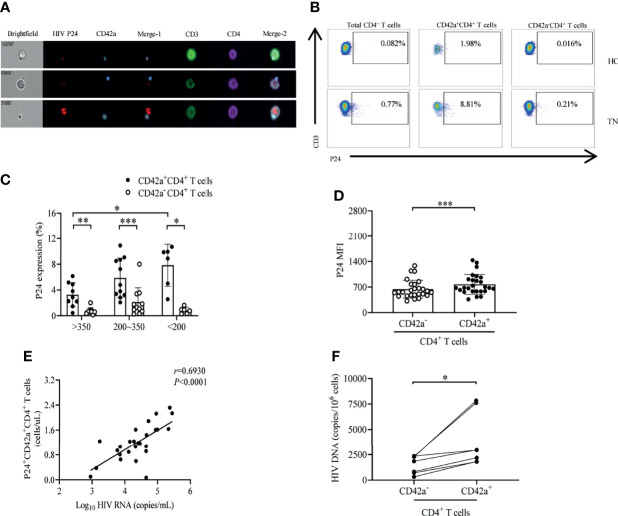
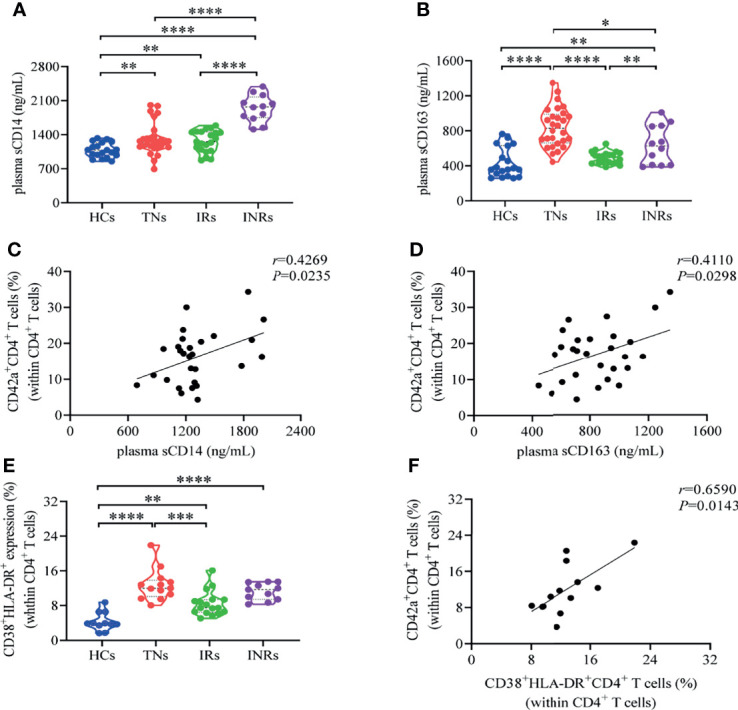
Chronic HIV-1 infection is associated with persistent inflammation, which contributes to disease progression. Platelet-T cell aggregates play a critical role in maintaining inflammation. However, the phenotypic characteristics and clinical significance of platelet-CD4+ T cell aggregates remain unclear in different HIV-infected populations. In this study, we quantified and characterized platelet-CD4+ T cell aggregates in the peripheral blood of treatment-naïve HIV-1-infected individuals (TNs), immunological responders to antiretroviral therapy (IRs), immunological non-responders to antiretroviral therapy (INRs), and healthy controls (HCs). Flow cytometry analysis and immunofluorescence microscopy showed increased platelet-CD4 + T cell aggregate formation in TNs compared to HCs during HIV-1 infection. However, the frequencies of platelet-CD4 + T cell aggregates decreased in IRs compared to TNs, but not in INRs, which have shown severe immunological dysfunction. Platelet-CD4 + T cell aggregate frequencies were positively correlated with HIV-1 viral load but negatively correlated with CD4 + T cell counts and CD4/CD8 ratios. Furthermore, we observed a higher expression of CD45RO, HIV co-receptors, HIV activation/exhaustion markers in platelet-CD4 + T cell aggregates, which was associated with HIV-1 permissiveness. High levels of caspase-1 and caspase-3, and low levels of Bcl-2 in platelet-CD4+ T cell aggregates imply the potential role in CD4+ T cell loss during HIV-1 infection. Furthermore, platelet-CD4 + T cell aggregates contained more HIV-1 gag viral protein and HIV-1 DNA than their platelet-free CD4 + T cell counterparts. The platelet-CD4 + T cell aggregate levels were positively correlated with plasma sCD163 and sCD14 levels. Our findings demonstrate that platelet-CD4 + T cell aggregate formation has typical characteristics of HIV-1 permissiveness and is related to immune activation during HIV-1 infection.
Keywords: HIV-1; T cell loss; infection; permissiveness; platelet-CD4+ T cell aggregates.
Copyright © 2021 Dai, Wu, Cui, Liao, Jiao, Zhang, Song, Fan, Zhang, He and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Increased platelet-CD8+ T-cell aggregates displaying high activation, exhaustion, and tendency to death correlate with disease progression in people with HIV-1.J Leukoc Biol. 2024 Jun 28;116(1):166-176. doi: 10.1093/jleuko/qiae048. J Leukoc Biol. 2024. PMID: 38450750
-
Markers of T Cell Exhaustion and Senescence and Their Relationship to Plasma TGF-β Levels in Treated HIV+ Immune Non-responders.Front Immunol. 2021 Mar 25;12:638010. doi: 10.3389/fimmu.2021.638010. eCollection 2021. Front Immunol. 2021. PMID: 33868264 Free PMC article.
-
Transcriptomic crosstalk between viral and host factors drives aberrant homeostasis of T-cell proliferation and cell death in HIV-infected immunological non-responders.J Infect. 2024 May;88(5):106151. doi: 10.1016/j.jinf.2024.106151. Epub 2024 Apr 4. J Infect. 2024. PMID: 38582127
-
T-cell exhaustion in HIV infection.Immunol Rev. 2019 Nov;292(1):149-163. doi: 10.1111/imr.12823. Immunol Rev. 2019. PMID: 31883174 Free PMC article. Review.
-
Platelets in HIV: A Guardian of Host Defence or Transient Reservoir of the Virus?Front Immunol. 2021 Apr 23;12:649465. doi: 10.3389/fimmu.2021.649465. eCollection 2021. Front Immunol. 2021. PMID: 33968041 Free PMC article. Review.
Cited by
-
Severe intestinal barrier damage in HIV-infected immunological non-responders.Heliyon. 2023 Oct 12;9(10):e20790. doi: 10.1016/j.heliyon.2023.e20790. eCollection 2023 Oct. Heliyon. 2023. PMID: 37876458 Free PMC article.
-
Alterations in circulating markers in HIV/AIDS patients with poor immune reconstitution: Novel insights from microbial translocation and innate immunity.Front Immunol. 2022 Oct 17;13:1026070. doi: 10.3389/fimmu.2022.1026070. eCollection 2022. Front Immunol. 2022. PMID: 36325329 Free PMC article. Review.
-
PSGL-1, a Strategic Biomarker for Pathological Conditions in HIV Infection: A Hypothesis Review.Viruses. 2023 Oct 31;15(11):2197. doi: 10.3390/v15112197. Viruses. 2023. PMID: 38005875 Free PMC article. Review.
-
Recent advances in poor HIV immune reconstitution: what will the future look like?Front Microbiol. 2023 Aug 7;14:1236460. doi: 10.3389/fmicb.2023.1236460. eCollection 2023. Front Microbiol. 2023. PMID: 37608956 Free PMC article. Review.
-
Platelet, a key regulator of innate and adaptive immunity.Front Med (Lausanne). 2023 Mar 10;10:1074878. doi: 10.3389/fmed.2023.1074878. eCollection 2023. Front Med (Lausanne). 2023. PMID: 36968817 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials