

Effect of increased alcohol consumption during COVID-19 pandemic on alcohol-associated liver disease: A modeling study
- PMID: 34878683
- PMCID: PMC9015640
- DOI: 10.1002/hep.32272
Effect of increased alcohol consumption during COVID-19 pandemic on alcohol-associated liver disease: A modeling study
Abstract
Background and aims: Alcohol consumption increased during the COVID-19 pandemic in 2020 in the United States. We projected the effect of increased alcohol consumption on alcohol-associated liver disease (ALD) and mortality.
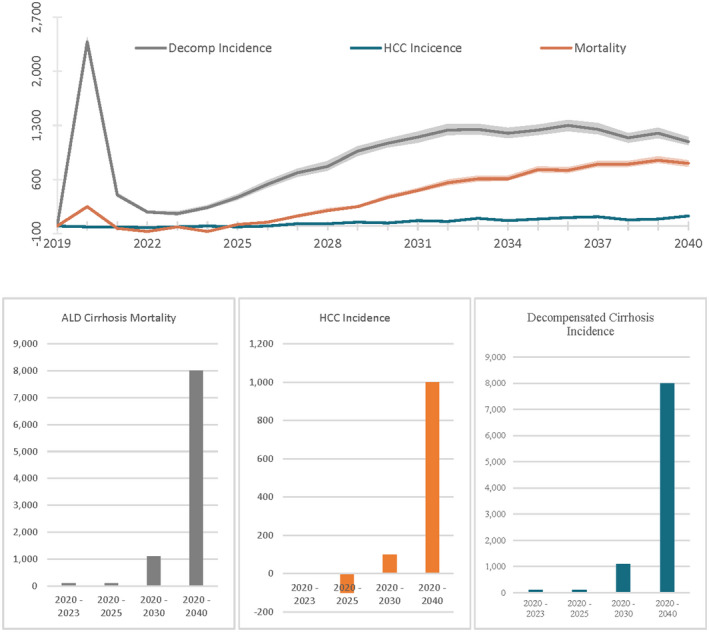
Approach and results: We extended a previously validated microsimulation model that estimated the short- and long-term effect of increased drinking during the COVID-19 pandemic in individuals in the United States born between 1920 and 2012. We modeled short- and long-term outcomes of current drinking patterns during COVID-19 (status quo) using survey data of changes in alcohol consumption in a nationally representative sample between February and November 2020. We compared these outcomes with a counterfactual scenario wherein no COVID-19 occurs and drinking patterns do not change. One-year increase in alcohol consumption during the COVID-19 pandemic is estimated to result in 8000 (95% uncertainty interval [UI], 7500-8600) additional ALD-related deaths, 18,700 (95% UI, 17,600-19,900) cases of decompensated cirrhosis, and 1000 (95% UI, 1000-1100) cases of HCC, and 8.9 million disability-adjusted life years between 2020 and 2040. Between 2020 and 2023, alcohol consumption changes due to COVID-19 will lead to 100 (100-200) additional deaths and 2800 (2700-2900) additional decompensated cirrhosis cases. A sustained increase in alcohol consumption for more than 1 year could result in additional morbidity and mortality.
Conclusions: A short-term increase in alcohol consumption during the COVID-19 pandemic can substantially increase long-term ALD-related morbidity and mortality. Our findings highlight the need for individuals and policymakers to make informed decisions to mitigate the impact of high-risk alcohol drinking in the United States.
© 2021 American Association for the Study of Liver Diseases.
Conflict of interest statement
Elliot Tapper has served as a consultant to Norvartis, Axcella, Kaleido, and Allergan; served on advisory boards for Takeda, Mallinckrodt, Rebiotix, and Bausch Health; and received unrestricted research grants from Gilead and Valeant. Jagpreet Chhatwal has served as a consultant to Novo Nordisk and partner at Value Analytics Labs. Turgay Ayer has served as a consultant to Merck and partner at Value Analytics Labs. No other author has a conflict of interest.
Figures



Similar articles
-
Modeling the impact of COVID-19 pandemic-driven increases in alcohol consumption on health outcomes and hospitalization costs in the United States.Addiction. 2023 Jan;118(1):48-60. doi: 10.1111/add.16018. Epub 2022 Aug 17. Addiction. 2023. PMID: 35915549 Free PMC article.
-
Projected prevalence and mortality associated with alcohol-related liver disease in the USA, 2019-40: a modelling study.Lancet Public Health. 2020 Jun;5(6):e316-e323. doi: 10.1016/S2468-2667(20)30062-1. Lancet Public Health. 2020. PMID: 32504584
-
Estimated projection of incidence and mortality of alcohol-related liver disease in China from 2022 to 2040: a modeling study.BMC Med. 2023 Jul 27;21(1):277. doi: 10.1186/s12916-023-02984-7. BMC Med. 2023. PMID: 37501074 Free PMC article.
-
Covid-19 and alcohol associated liver disease.Dig Liver Dis. 2022 Nov;54(11):1459-1468. doi: 10.1016/j.dld.2022.07.007. Epub 2022 Aug 4. Dig Liver Dis. 2022. PMID: 35933291 Free PMC article. Review.
-
Intersection of Coronavirus Disease 2019 and Alcohol-associated Liver Disease: A Review of Emerging Trends and Implications.Clin Ther. 2023 Dec;45(12):1164-1170. doi: 10.1016/j.clinthera.2023.08.019. Epub 2023 Sep 26. Clin Ther. 2023. PMID: 37758533 Review.
Cited by
-
COVID-19-associated liver injury: Clinical characteristics, pathophysiological mechanisms and treatment management.Biomed Pharmacother. 2022 Oct;154:113568. doi: 10.1016/j.biopha.2022.113568. Epub 2022 Aug 17. Biomed Pharmacother. 2022. PMID: 36029543 Free PMC article. Review.
-
Association between alcohol-associated cirrhosis and inpatient complications among COVID-19 patients: A propensity-matched analysis from the United States.World J Virol. 2023 Sep 25;12(4):221-232. doi: 10.5501/wjv.v12.i4.221. World J Virol. 2023. PMID: 37970569 Free PMC article.
-
Global epidemiology of cirrhosis - aetiology, trends and predictions.Nat Rev Gastroenterol Hepatol. 2023 Jun;20(6):388-398. doi: 10.1038/s41575-023-00759-2. Epub 2023 Mar 28. Nat Rev Gastroenterol Hepatol. 2023. PMID: 36977794 Free PMC article. Review.
-
Acute Alcohol-Associated Hepatitis in the COVID-19 Pandemic - a Structured Review.Curr Transplant Rep. 2022;9(4):227-239. doi: 10.1007/s40472-022-00387-w. Epub 2022 Nov 21. Curr Transplant Rep. 2022. PMID: 36466960 Free PMC article. Review.
-
Higher-Than-Expected Burden of Alcohol-Related Liver Diseases During COVID-19 Pandemic in the USA, with a Tapering Trend.J Gen Intern Med. 2024 Sep;39(12):2133-2141. doi: 10.1007/s11606-023-08594-6. Epub 2024 Jan 16. J Gen Intern Med. 2024. PMID: 38228988
References
-
- Barbosa C, Karriker‐Jaffe K, Dowd W. One year later: how have american drinking habits changed during the COVID‐19 pandemic. RTI International; 2021. https://www.rti.org/sites/default/files/fy21_covid_drinking_webinar_slid.... Accessed 30 Aug 2021.
-
- IZEA . Coronavirus impacts on alcohol & social media consumption. IZEA; 2020.
-
- Drizly . How alcohol ecommerce sales are being impacted across North America. April 27, 2020; 2021. https://drizly.com/article/education/extras/how‐alcohol‐ecommerce‐sales‐.... Accessed 27 Apr 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
