

SARS-CoV-2 and influenza virus coinfection among patients with severe acute respiratory infection during the first wave of COVID-19 pandemic in Bangladesh: a hospital-based descriptive study
- PMID: 34845073
- PMCID: PMC8634662
- DOI: 10.1136/bmjopen-2021-053768
SARS-CoV-2 and influenza virus coinfection among patients with severe acute respiratory infection during the first wave of COVID-19 pandemic in Bangladesh: a hospital-based descriptive study
Abstract
Objective: To estimate the proportion of SARS-CoV-2 and influenza virus coinfection among severe acute respiratory infection (SARI) cases-patients during the first wave of COVID-19 pandemic in Bangladesh.
Design: Descriptive study.
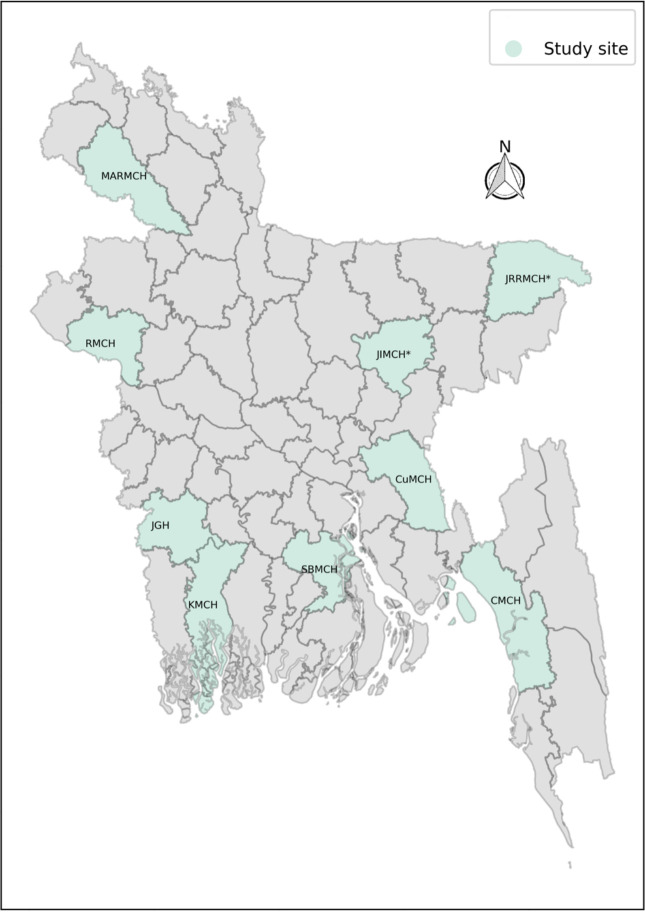
Setting: Nine tertiary level hospitals across Bangladesh.
Participants: Patients admitted as SARI (defined as cases with subjective or measured fever of ≥38 C° and cough with onset within the last 10 days and requiring hospital admission) case-patients.
Primary and secondary outcomes: Proportion of SARS-CoV-2 and influenza virus coinfection and proportion of mortality among SARI case-patients.
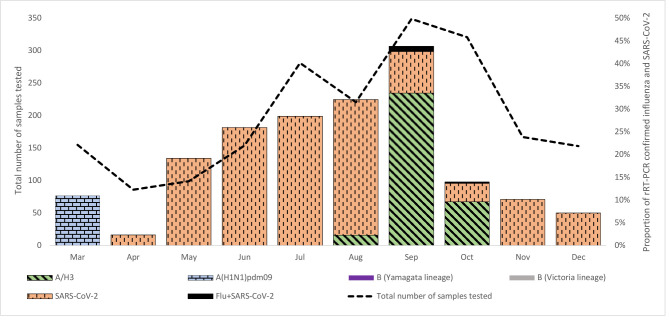
Results: We enrolled 1986 SARI case-patients with a median age: 28 years (IQR: 1.2-53 years), and 67.6% were male. Among them, 285 (14.3%) were infected with SARS-CoV-2; 175 (8.8%) were infected with the influenza virus, and five (0.3%) were coinfected with both viruses. There was a non-appearance of influenza during the usual peak season (May to July) in Bangladesh. SARS-CoV-2 infection was significantly more associated with diabetes (14.0% vs 5.9%, p<0.001) and hypertension (26.7% vs 11.5%, p<0.001). But influenza among SARI case-patients was significantly less associated with diabetes (4.0% vs 7.4%, p=0.047) and hypertension (5.7% vs 14.4%, p=0.001). The proportion of in-hospital deaths among SARS-CoV-2 infected SARI case-patients were higher (10.9% (n=31) vs 4.4% (n=75), p<0.001) than those without SARS-CoV-2 infection; the proportion of postdischarge deaths within 30 days was also higher (9.1% (n=25) vs 4.6% (n=74), p=0.001) among SARS-CoV-2 infected SARI case-patients than those without infection. No in-hospital mortality or postdischarge mortality was registered among the five coinfected SARI case-patients.
Conclusions: Our findings suggest that coinfection with SARS-CoV-2 and influenza virus was not very common and had less disease severity considering mortality in Bangladesh. There was no circulating influenza virus during the influenza peak season during the COVID-19 pandemic in 2020. Future studies are warranted for further exploration.
Keywords: COVID-19; epidemiology; infectious diseases.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report.Viruses. 2022 Mar 17;14(3):627. doi: 10.3390/v14030627. Viruses. 2022. PMID: 35337033 Free PMC article.
-
Characterizing deaths among adult patients with severe acute respiratory infection: during the pre- and COVID-19 pandemic periods in Bangladesh, 2018-2022.Trop Med Health. 2023 Dec 19;51(1):70. doi: 10.1186/s41182-023-00565-1. Trop Med Health. 2023. PMID: 38115037 Free PMC article.
-
Clinical and Epidemiological Features of SARS-CoV-2 Patients in SARI Ward of a Tertiary Care Centre in New Delhi.J Assoc Physicians India. 2020 Jul;68(7):19-26. J Assoc Physicians India. 2020. PMID: 32602676
-
Co-infection of SARS-COV-2 and Influenza A Virus: A Case Series and Fast Review.Curr Med Sci. 2021 Feb;41(1):51-57. doi: 10.1007/s11596-021-2317-2. Epub 2021 Feb 13. Curr Med Sci. 2021. PMID: 33582905 Free PMC article. Review.
-
Impact of Coinfection With SARS-CoV-2 and Influenza on Disease Severity: A Systematic Review and Meta-Analysis.Front Public Health. 2021 Dec 10;9:773130. doi: 10.3389/fpubh.2021.773130. eCollection 2021. Front Public Health. 2021. PMID: 34957025 Free PMC article. Review.
Cited by
-
Epidemiology, Disease Severity and Outcome of Severe Acute Respiratory Syndrome Coronavirus 2 and Influenza Viruses Coinfection Seen at Egypt Integrated Acute Respiratory Infections Surveillance, 2020-2022.Can J Infect Dis Med Microbiol. 2022 Nov 17;2022:7497500. doi: 10.1155/2022/7497500. eCollection 2022. Can J Infect Dis Med Microbiol. 2022. PMID: 36437892 Free PMC article.
-
Co-existence and co-infection of influenza A viruses and coronaviruses: Public health challenges.Innovation (Camb). 2022 Sep 13;3(5):100306. doi: 10.1016/j.xinn.2022.100306. Epub 2022 Aug 17. Innovation (Camb). 2022. PMID: 35992368 Free PMC article. Review.
-
The impact of COVID-19 and COVID vaccination on cardiovascular outcomes.Eur Heart J Suppl. 2023 Feb 14;25(Suppl A):A42-A49. doi: 10.1093/eurheartjsupp/suac123. eCollection 2023 Feb. Eur Heart J Suppl. 2023. PMID: 36937372 Free PMC article.
-
SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report.Viruses. 2022 Mar 17;14(3):627. doi: 10.3390/v14030627. Viruses. 2022. PMID: 35337033 Free PMC article.
-
In-silico modelling studies of 5-benzyl-4-thiazolinone derivatives as influenza neuraminidase inhibitors via 2D-QSAR, 3D-QSAR, molecular docking, and ADMET predictions.Heliyon. 2022 Aug 8;8(8):e10101. doi: 10.1016/j.heliyon.2022.e10101. eCollection 2022 Aug. Heliyon. 2022. Retraction in: Heliyon. 2023 Aug 02;9(8):e18877. doi: 10.1016/j.heliyon.2023.e18877. PMID: 36016519 Free PMC article. Retracted.
References
-
- Hampson AW. Vaccines for pandemic influenza. The history of our current vaccines, their limitations and the requirements to deal with a pandemic threat. Ann Acad Med Singap 2008;37:510. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous