

Predicted Cure and Survival Among Transplant Recipients With a Previous Cancer Diagnosis
- PMID: 34678077
- PMCID: PMC8677988
- DOI: 10.1200/JCO.21.01195
Predicted Cure and Survival Among Transplant Recipients With a Previous Cancer Diagnosis
Abstract
Purpose: A previous cancer diagnosis is a negative consideration in evaluating patients for possible solid organ transplantation. Statistical models may improve selection of patients with cancer evaluated for transplantation.
Methods: We fitted statistical cure models for patients with cancer in the US general population using data from 13 cancer registries. Patients subsequently undergoing solid organ transplantation were identified through the Scientific Registry of Transplant Recipients. We estimated cure probabilities at diagnosis (for all patients with cancer) and transplantation (transplanted patients). We used Cox regression to assess associations of cure probability at transplantation with subsequent cancer-specific mortality.
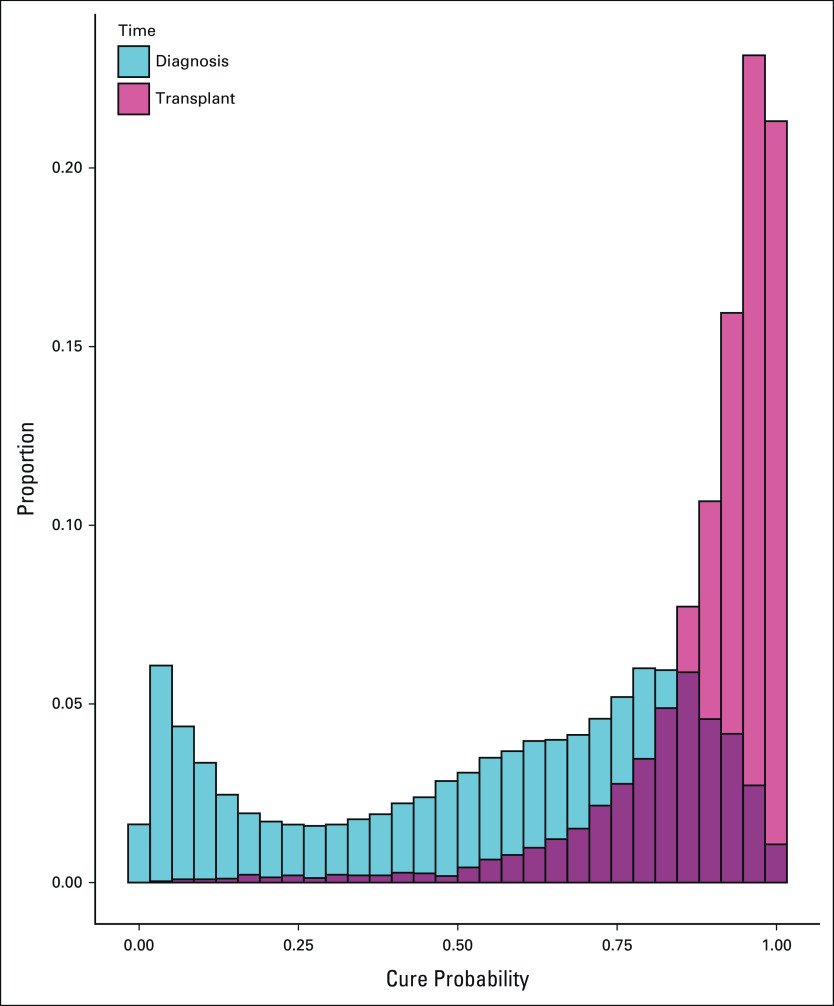
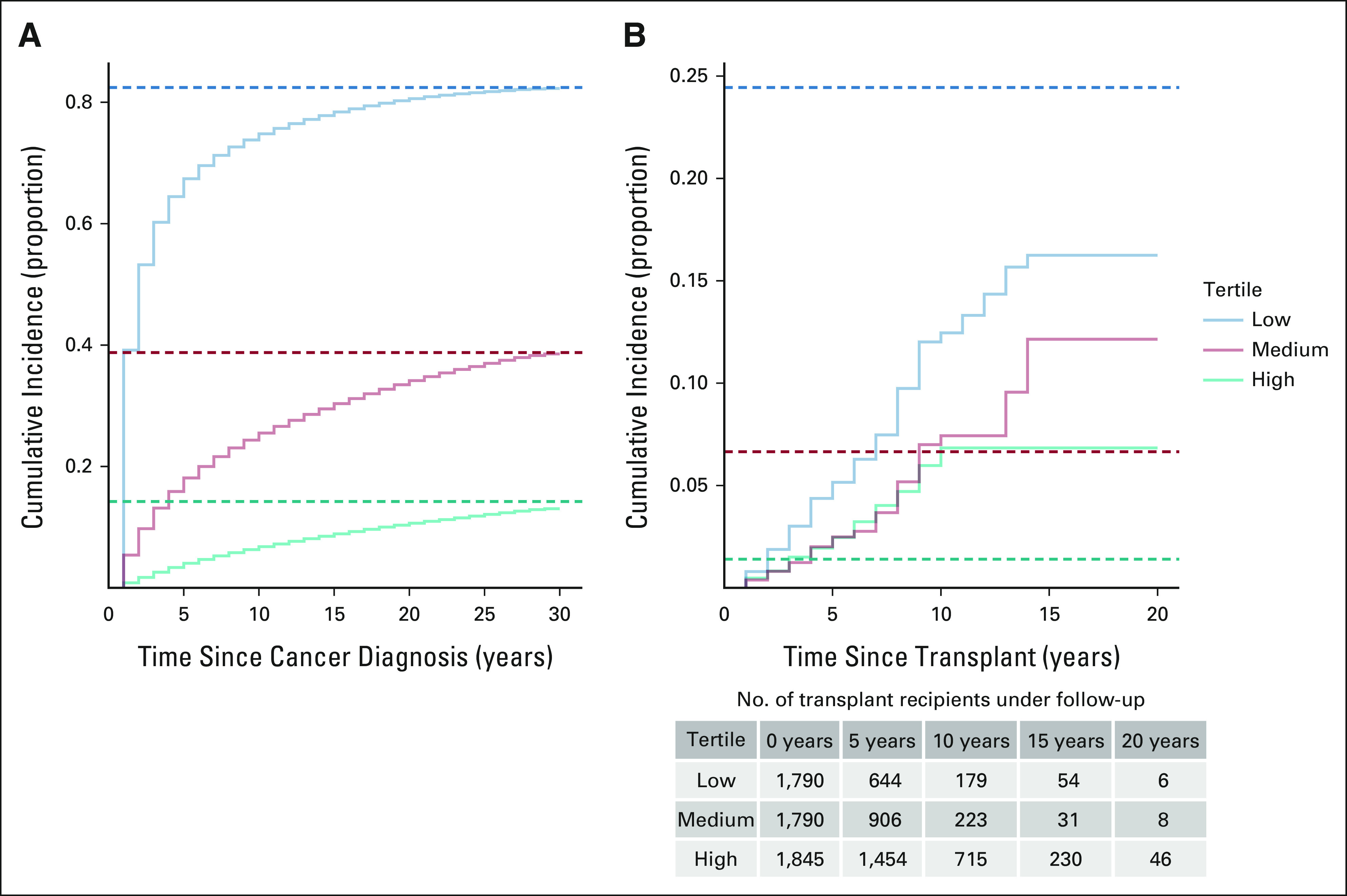
Results: Among 10,524,326 patients with 17 cancer types in the general population, the median cure probability at diagnosis was 62%. Of these patients, 5,425 (0.05%) subsequently underwent solid organ transplantation and their median cure probability at transplantation was 94% (interquartile range, 86%-98%). Compared with the tertile of transplanted patients with highest cure probability, those in the lowest tertile more frequently had lung or breast cancers and less frequently colorectal, testicular, or thyroid cancers; more frequently had advanced-stage cancer; were older (median 57 v 51 years); and were transplanted sooner after cancer diagnosis (median 3.6 v 8.6 years). Patients in the low-cure probability tertile had increased cancer-specific mortality after transplantation (adjusted hazard ratio, 2.08; 95% CI, 1.48 to 2.93; v the high tertile), whereas those in the middle tertile did not differ.
Conclusion: Patients with cancer who underwent solid organ transplantation exhibited high cure probabilities, reflecting selection on the basis of existing guidelines and clinical judgment. Nonetheless, there was a range of cure probabilities among transplanted patients and low probability predicted increased cancer-specific mortality after transplantation. Cure probabilities may facilitate guideline development and evaluating individual patients for transplantation.
Conflict of interest statement
Figures
Similar articles
-
Cure models, survival probabilities, and solid organ transplantation for patients with colorectal cancer.Am J Transplant. 2024 Sep 5:S1600-6135(24)00527-6. doi: 10.1016/j.ajt.2024.08.018. Online ahead of print. Am J Transplant. 2024. PMID: 39182612
-
Solid Organ Transplantation and Survival among Individuals with a History of Cancer.Cancer Epidemiol Biomarkers Prev. 2021 Jul;30(7):1312-1319. doi: 10.1158/1055-9965.EPI-21-0044. Epub 2021 Apr 29. Cancer Epidemiol Biomarkers Prev. 2021. PMID: 33926864 Free PMC article.
-
Survival after a cancer diagnosis among solid organ transplant recipients in the United States.Cancer. 2019 Mar 15;125(6):933-942. doi: 10.1002/cncr.31782. Epub 2019 Jan 9. Cancer. 2019. PMID: 30624768 Free PMC article.
-
Recipient donor sex combinations in solid organ transplantation and impact on clinical outcome: A scoping review.Clin Transplant. 2024 May;38(5):e15312. doi: 10.1111/ctr.15312. Clin Transplant. 2024. PMID: 38678586 Review.
-
Outcomes of Solid Organ Transplant Recipients With Preexisting Malignancies in Remission: A Systematic Review and Meta-Analysis.Transplantation. 2017 Mar;101(3):471-481. doi: 10.1097/TP.0000000000001192. Transplantation. 2017. PMID: 27101077 Review.
Cited by
-
Prior cancer history and suitability for kidney transplantation.Clin Kidney J. 2023 Jun 28;16(11):1908-1916. doi: 10.1093/ckj/sfad141. eCollection 2023 Nov. Clin Kidney J. 2023. PMID: 37915927 Free PMC article. Review.
-
Use of Systemic Therapies for Treatment of Psoriasis in Patients with a History of Treated Solid Tumours: Inference-Based Guidance from a Multidisciplinary Expert Panel.Dermatol Ther (Heidelb). 2023 Apr;13(4):867-889. doi: 10.1007/s13555-023-00905-3. Epub 2023 Mar 16. Dermatol Ther (Heidelb). 2023. PMID: 36929121 Free PMC article.
-
Mortality among solid organ transplant recipients with a pretransplant cancer diagnosis.Am J Transplant. 2023 Feb;23(2):257-264. doi: 10.1016/j.ajt.2022.11.006. Epub 2023 Jan 12. Am J Transplant. 2023. PMID: 36804133 Free PMC article.
References
-
- Grulich AE, van Leeuwen MT, Falster MO, et al. : Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 370:59-67, 2007 - PubMed
-
- Hart A, Engels EA: Balancing uncertain risks in candidates for solid organ transplantation with a history of malignancy: Who is safe to transplant? Am J Transplant 21:447-448, 2020 - PubMed
-
- Faitot F, Michard B, Artzner T: Organ allocation in the age of the algorithm: Avoiding futile transplantation—Utility in allocation. Curr Opin Organ Transplant 25:305-309, 2020 - PubMed
Publication types
MeSH terms
Grants and funding
- 75N99021D00009/OF/ORFDO NIH HHS/United States
- HHSN261201000037C/CA/NCI NIH HHS/United States
- N01PC35143/CA/NCI NIH HHS/United States
- U58 DP003875/DP/NCCDPHP CDC HHS/United States
- HHSN261201000036C/CA/NCI NIH HHS/United States
- N01PC35137/CA/NCI NIH HHS/United States
- U58 DP003920/DP/NCCDPHP CDC HHS/United States
- U58 DP000807/DP/NCCDPHP CDC HHS/United States
- N01PC35142/CA/NCI NIH HHS/United States
- U58 DP003933/DP/NCCDPHP CDC HHS/United States
- HHSN261201000035I/CA/NCI NIH HHS/United States
- U58 DP000848/DP/NCCDPHP CDC HHS/United States
- U58 DP003883/DP/NCCDPHP CDC HHS/United States
- HHSN261201000035C/CA/NCI NIH HHS/United States
- 75N96021D00009/ES/NIEHS NIH HHS/United States
- HHSN261201300071C/CA/NCI NIH HHS/United States
- HHSN261201000034C/CA/NCI NIH HHS/United States
- U58 DP003921/DP/NCCDPHP CDC HHS/United States
- N01PC35139/CA/NCI NIH HHS/United States
- HHSN261201800002C/CA/NCI NIH HHS/United States
- HHSN261201300011C/CA/NCI NIH HHS/United States
- U58 DP000824/DP/NCCDPHP CDC HHS/United States
- HHSN261201800002B/CA/NCI NIH HHS/United States
- 75N92021D00009/HL/NHLBI NIH HHS/United States
- 75N90021D00009/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
