

Analyses of child cardiometabolic phenotype following assisted reproductive technologies using a pragmatic trial emulation approach
- PMID: 34556649
- PMCID: PMC8460697
- DOI: 10.1038/s41467-021-25899-4
Analyses of child cardiometabolic phenotype following assisted reproductive technologies using a pragmatic trial emulation approach
Abstract
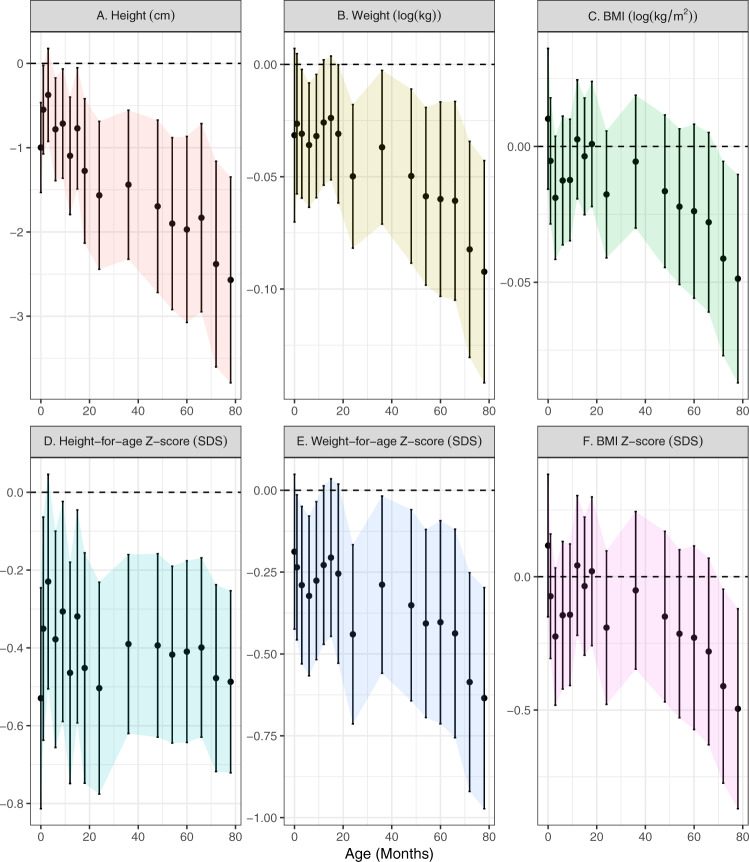
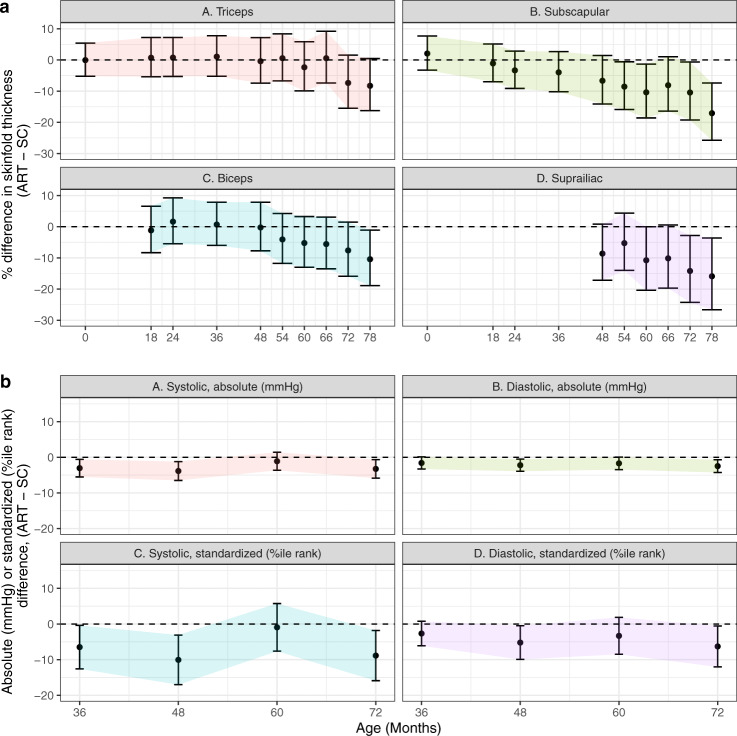
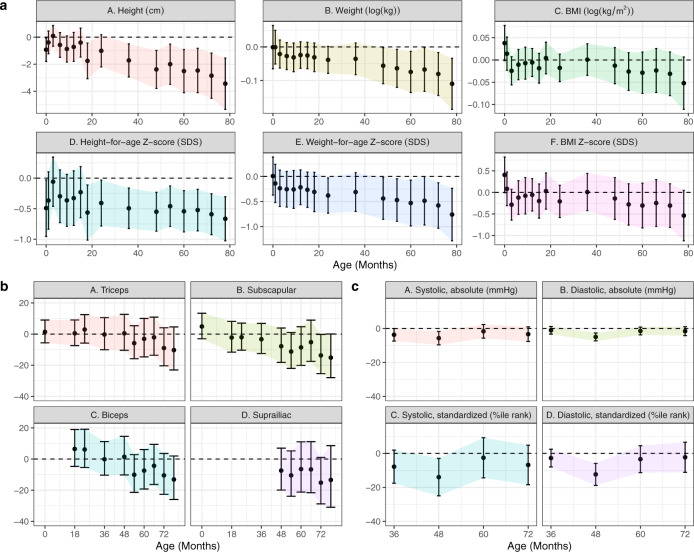
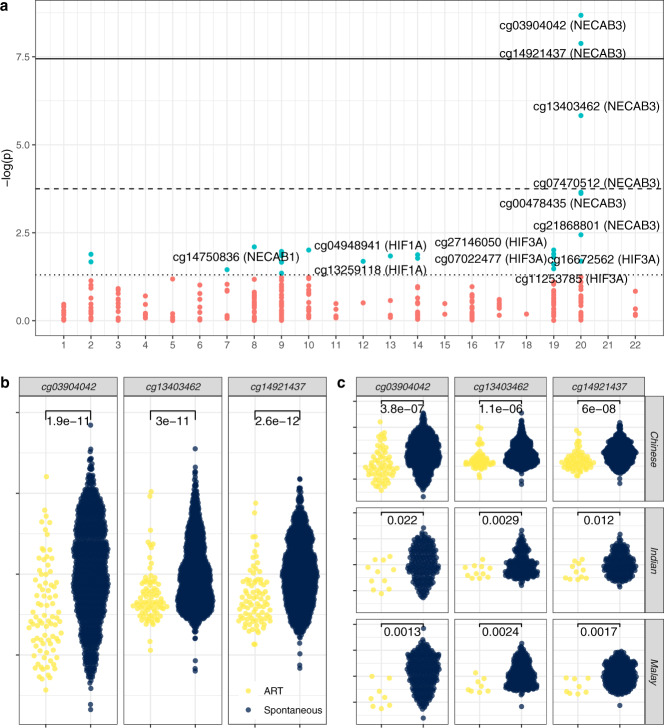
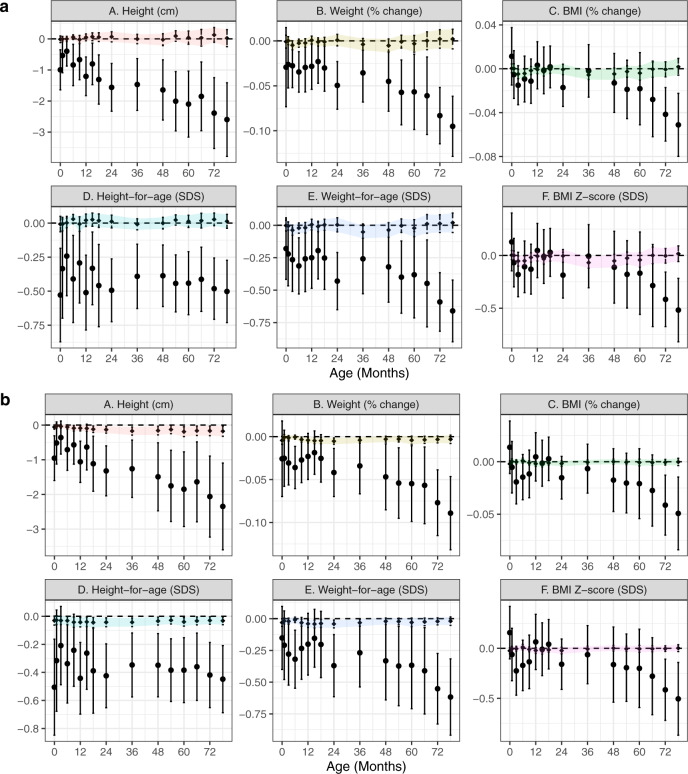
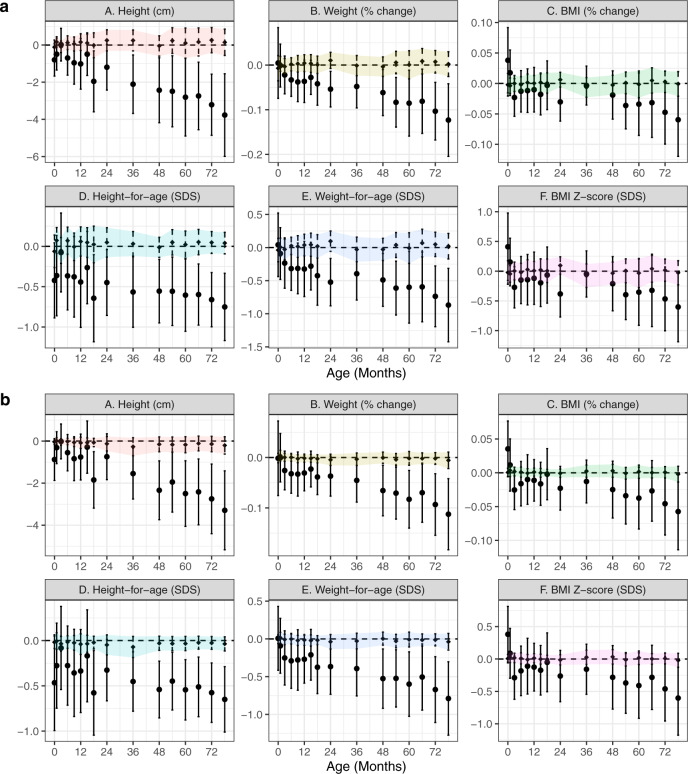
Assisted reproductive technologies (ART) are increasingly used, however little is known about the long-term health of ART-conceived offspring. Weak selection of comparison groups and poorly characterized mechanisms impede current understanding. In a prospective cohort (Growing Up in Singapore Towards healthy Outcomes; GUSTO; Clinical Trials ID: NCT01174875) including 83 ART-conceived and 1095 spontaneously-conceived singletons, we estimate effects of ART on anthropometry, blood pressure, serum metabolic biomarkers, and cord tissue DNA methylation by emulating a pragmatic trial supported by machine learning-based estimators. We find ART-conceived children to be shorter (-0.5 SD [95% CI: -0.7, -0.2]), lighter (-0.6 SD [-0.9, -0.3]) and have lower skinfold thicknesses (e.g. -14% [-24%, -3%] suprailiac), and blood pressure (-3 mmHg [-6, -0.5] systolic) at 6-6.5 years, with no strong differences in metabolic biomarkers. Differences are not explained by parental anthropometry or comorbidities, polygenic risk score, breastfeeding, or illnesses. Our simulations demonstrate ART is strongly associated with lower NECAB3 DNA methylation, with negative control analyses suggesting these estimates are unbiased. However, methylation changes do not appear to mediate observed differences in child phenotype.
© 2021. The Author(s).
Conflict of interest statement
Y.S.C., S.Y.C., and K.M.G. have received reimbursement for speaking at conferences sponsored by companies selling nutritional products, and are part of an academic consortium that has received research funding from Abbott Nutrition, Nestec, and Danone. The remaining authors declare no competing interests.
Figures
Similar articles
-
Assessment of Cardiovascular Health of Children Ages 6 to 10 Years Conceived by Assisted Reproductive Technology.JAMA Netw Open. 2021 Nov 1;4(11):e2132602. doi: 10.1001/jamanetworkopen.2021.32602. JAMA Netw Open. 2021. PMID: 34735014 Free PMC article.
-
Study protocol for a Developmental Epidemiological Study of Children born through Reproductive Technologies (DESCRT).Hum Reprod Open. 2023 May 5;2023(2):hoad013. doi: 10.1093/hropen/hoad013. eCollection 2023. Hum Reprod Open. 2023. PMID: 37265937 Free PMC article. Review.
-
Comparison of the cardiometabolic profiles of adolescents conceived through ART with those of a non-ART cohort.Hum Reprod. 2022 Jul 30;37(8):1880-1895. doi: 10.1093/humrep/deac122. Hum Reprod. 2022. PMID: 35640037 Free PMC article.
-
Cohort profile: The Growing Up Healthy Study (GUHS)-A prospective and observational cohort study investigating the long-term health outcomes of offspring conceived after assisted reproductive technologies.PLoS One. 2022 Jul 22;17(7):e0272064. doi: 10.1371/journal.pone.0272064. eCollection 2022. PLoS One. 2022. PMID: 35867723 Free PMC article.
-
Clinical review of 24-35 year olds conceived with and without in vitro fertilization: study protocol.Reprod Health. 2017 Sep 20;14(1):117. doi: 10.1186/s12978-017-0377-3. Reprod Health. 2017. PMID: 28931409 Free PMC article. Review.
Cited by
-
Deciphering the role of immune cell composition in epigenetic age acceleration: Insights from cell-type deconvolution applied to human blood epigenetic clocks.Aging Cell. 2024 Mar;23(3):e14071. doi: 10.1111/acel.14071. Epub 2023 Dec 25. Aging Cell. 2024. PMID: 38146185 Free PMC article.
-
Association of Assisted Reproductive Technology With Offspring Growth and Adiposity From Infancy to Early Adulthood.JAMA Netw Open. 2022 Jul 1;5(7):e2222106. doi: 10.1001/jamanetworkopen.2022.22106. JAMA Netw Open. 2022. PMID: 35881399 Free PMC article.
-
Epigenetic Risks of Medically Assisted Reproduction.J Clin Med. 2022 Apr 12;11(8):2151. doi: 10.3390/jcm11082151. J Clin Med. 2022. PMID: 35456243 Free PMC article. Review.
-
Long-term cardiometabolic health in people born after assisted reproductive technology: a multi-cohort analysis.Eur Heart J. 2023 Apr 21;44(16):1464-1473. doi: 10.1093/eurheartj/ehac726. Eur Heart J. 2023. PMID: 36740401 Free PMC article.
-
Learning across diverse biomedical data modalities and cohorts: Challenges and opportunities for innovation.Patterns (N Y). 2024 Jan 17;5(2):100913. doi: 10.1016/j.patter.2023.100913. eCollection 2024 Feb 9. Patterns (N Y). 2024. PMID: 38370129 Free PMC article. Review.
References
-
- Teo, J. More Singapore couples getting help to conceive. The Straits Times. 2016 March 22. https://www.straitstimes.com/singapore/health/more-singapore-couples-get...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
