

Healthcare-associated COVID-19 in England: A national data linkage study
- PMID: 34474055
- PMCID: PMC8404398
- DOI: 10.1016/j.jinf.2021.08.039
Healthcare-associated COVID-19 in England: A national data linkage study
Abstract
Objectives: Nosocomial transmission was an important aspect of SARS-CoV-1 and MERS-CoV outbreaks. Healthcare-associated SARS-CoV-2 infection has been reported in single and multi-site hospital-based studies in England, but not nationally.
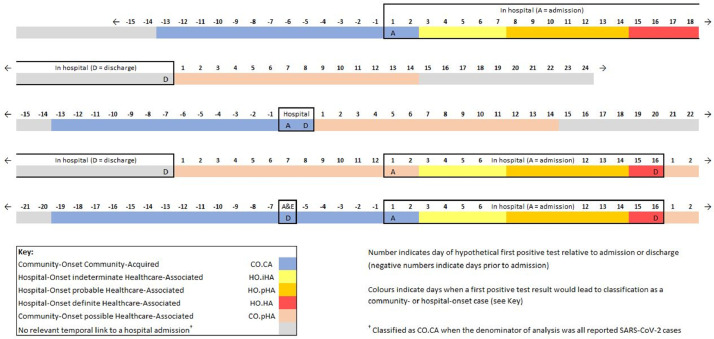
Methods: Admission records for all hospitals in England were linked to SARS-CoV-2 national test data for the period 01/03/2020 to 31/08/2020. Case definitions were: community-onset community-acquired, first positive test <14 days pre-admission, up to day 2 of admission; hospital-onset indeterminate healthcare-associated, first positive on day 3-7; hospital-onset probable healthcare-associated, first positive on day 8-14; hospital-onset definite healthcare-associated, first positive from day 15 of admission until discharge; community-onset possible healthcare-associated, first positive test ≤14 days post-discharge.
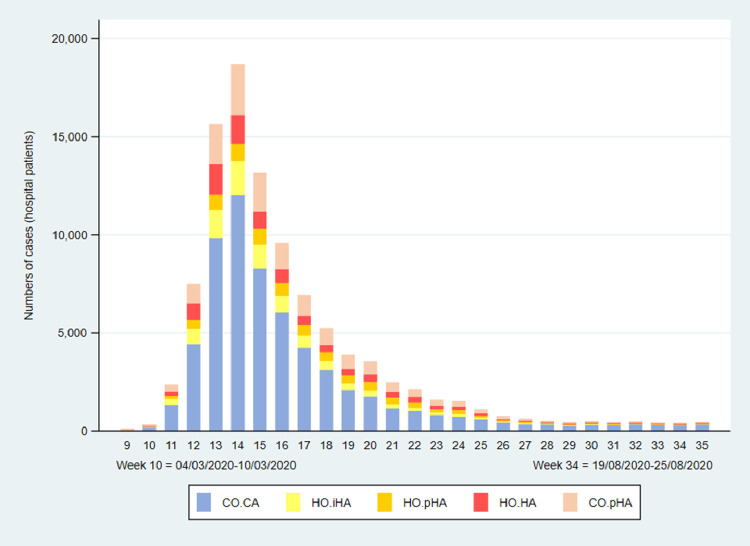
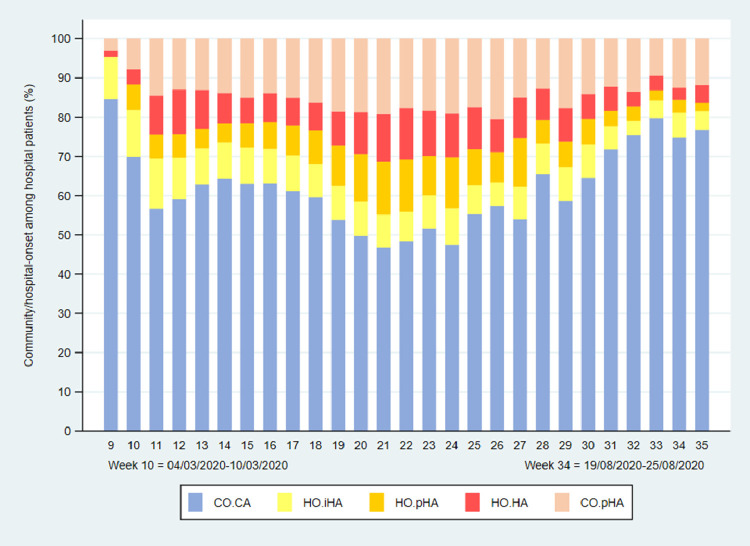
Results: One-third (34.4%, 100,859/293,204) of all laboratory-confirmed COVID-19 cases were linked to a hospital record. Hospital-onset probable and definite cases represented 5.3% (15,564/293,204) of all laboratory-confirmed cases and 15.4% (15,564/100,859) of laboratory-confirmed cases among hospital patients. Community-onset community-acquired and community-onset possible healthcare-associated cases represented 86.5% (253,582/293,204) and 5.1% (14,913/293,204) of all laboratory-confirmed cases, respectively.
Conclusions: Up to 1 in 6 SARS-CoV-2 infections among hospitalised patients with COVID-19 in England during the first 6 months of the pandemic could be attributed to nosocomial transmission, but these represent less than 1% of the estimated 3 million COVID-19 cases in this period.
Keywords: COVID-19; Community-onset infection; Healthcare-associated infection; Sars-CoV-2.
Copyright © 2021. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest None.
Figures
Similar articles
-
The contribution of hospital-acquired infections to the COVID-19 epidemic in England in the first half of 2020.BMC Infect Dis. 2022 Jun 18;22(1):556. doi: 10.1186/s12879-022-07490-4. BMC Infect Dis. 2022. PMID: 35717168 Free PMC article.
-
A new method for near real-time, nationwide surveillance of nosocomial COVID-19 in Norway: providing data at all levels of the healthcare system, March 2020 to March 2022.Euro Surveill. 2023 Mar;28(12):2200493. doi: 10.2807/1560-7917.ES.2023.28.12.2200493. Euro Surveill. 2023. PMID: 36951784 Free PMC article.
-
Assessment of Hospital-Onset SARS-CoV-2 Infection Rates and Testing Practices in the US, 2020-2022.JAMA Netw Open. 2023 Aug 1;6(8):e2329441. doi: 10.1001/jamanetworkopen.2023.29441. JAMA Netw Open. 2023. PMID: 37639273 Free PMC article.
-
Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection.Cochrane Database Syst Rev. 2022 Jul 22;7(7):CD013705. doi: 10.1002/14651858.CD013705.pub3. Cochrane Database Syst Rev. 2022. PMID: 35866452 Free PMC article. Review.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses.Cochrane Database Syst Rev. 2023 Jan 30;1(1):CD006207. doi: 10.1002/14651858.CD006207.pub6. Cochrane Database Syst Rev. 2023. PMID: 36715243 Free PMC article. Review.
Cited by
-
Evaluating pooled testing for asymptomatic screening of healthcare workers in hospitals.BMC Infect Dis. 2023 Dec 21;23(1):900. doi: 10.1186/s12879-023-08881-x. BMC Infect Dis. 2023. PMID: 38129789 Free PMC article.
-
Transmission of community- and hospital-acquired SARS-CoV-2 in hospital settings in the UK: A cohort study.PLoS Med. 2021 Oct 12;18(10):e1003816. doi: 10.1371/journal.pmed.1003816. eCollection 2021 Oct. PLoS Med. 2021. PMID: 34637439 Free PMC article.
-
The contribution of hospital-acquired infections to the COVID-19 epidemic in England in the first half of 2020.BMC Infect Dis. 2022 Jun 18;22(1):556. doi: 10.1186/s12879-022-07490-4. BMC Infect Dis. 2022. PMID: 35717168 Free PMC article.
-
The impact of testing and infection prevention and control strategies on within-hospital transmission dynamics of COVID-19 in English hospitals.Philos Trans R Soc Lond B Biol Sci. 2021 Jul 19;376(1829):20200268. doi: 10.1098/rstb.2020.0268. Epub 2021 May 31. Philos Trans R Soc Lond B Biol Sci. 2021. PMID: 34053255 Free PMC article.
-
The effectiveness and efficiency of asymptomatic SARS-CoV-2 testing strategies for patient and healthcare workers within acute NHS hospitals during an omicron-like period.BMC Infect Dis. 2024 Jan 8;24(1):64. doi: 10.1186/s12879-023-08948-9. BMC Infect Dis. 2024. PMID: 38191324 Free PMC article.
References
-
- DELVE Initiative . The Royal Society; London: 2020. DELVE Scoping Report on Hospital and Health Care Acquisition of COVID-19 and its Control.https://rs-delve.github.io/reports/2020/07/06/nosocomial-scoping-report....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
