

Immune Microenvironment Landscape in CNS Tumors and Role in Responses to Immunotherapy
- PMID: 34440802
- PMCID: PMC8393758
- DOI: 10.3390/cells10082032
Immune Microenvironment Landscape in CNS Tumors and Role in Responses to Immunotherapy
Abstract
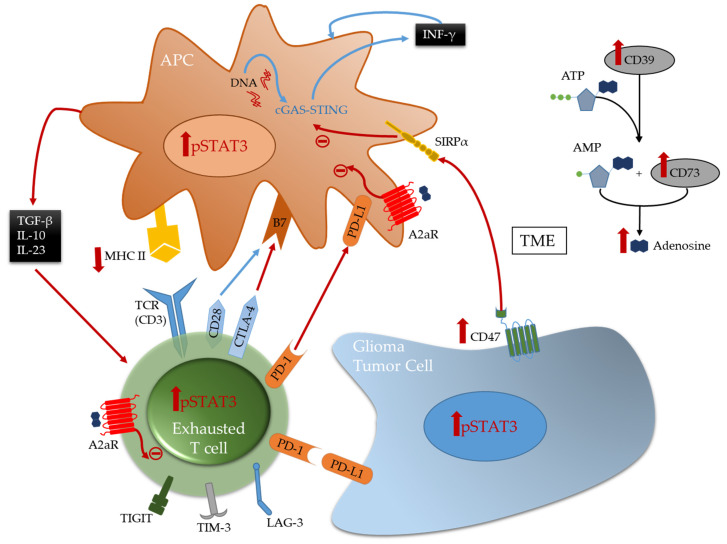
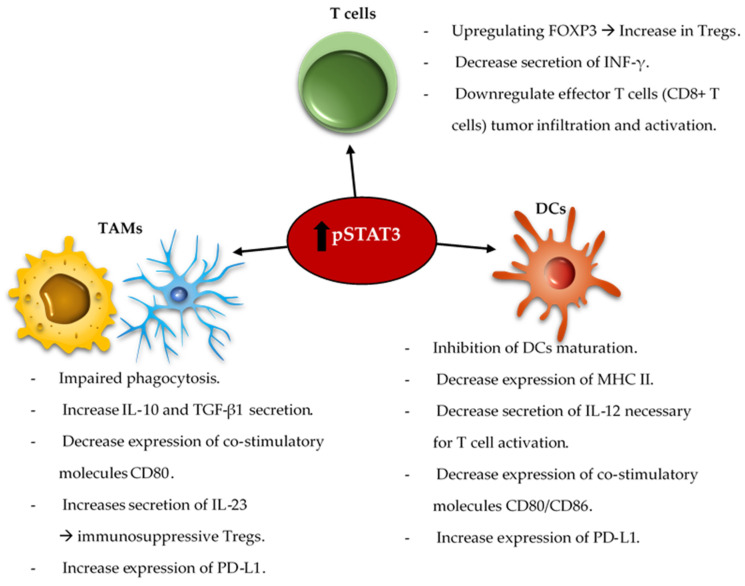
Despite the important evolution of immunotherapeutic agents, brain tumors remain, in general, refractory to immune therapeutics. Recent discoveries have revealed that the glioma microenvironment includes a wide variety of immune cells in various states that play an important role in the process of tumorigenesis. Anti-tumor immune activity may be occurring or induced in immunogenic hot spots or at the invasive edge of central nervous system (CNS) tumors. Understanding the complex heterogeneity of the immune microenvironment in gliomas will likely be the key to unlocking the full potential of immunotherapeutic strategies. An essential consideration will be the induction of immunological effector responses in the setting of the numerous aspects of immunosuppression and evasion. As such, immune therapeutic combinations are a fundamental objective for clinical studies in gliomas. Through immune profiling conducted on immune competent murine models of glioma and ex vivo human glioma tissue, we will discuss how the frequency, distribution of immune cells within the microenvironment, and immune modulatory processes, may be therapeutically modulated to lead to clinical benefits.
Keywords: CNS metastasis; T cells; glioma; immune checkpoints; immune composition; immune therapy; tumor associated macrophages/microglia; tumor microenvironment.
Conflict of interest statement
M.K. reports personal fees from Ipsen, Pfizer Roche, and Jackson Laboratory for Genomic Medicine and research funding paid to his institution from Specialized Therapeutics, all outside the submitted work. Research funding from AbbVie and Bristol-Myers Squibb were paid to his institution for glioblastoma research. A.B.H. serves on the advisory boards of Caris Life Sciences and WCG Oncology, receives royalties on licensed intellectual property from Celldex Therapeutics and DNAtrix, and receives research support from Celularity, Carthera, Codiak, and Moleculin. The other authors declare no conflict of interest.
Figures
Similar articles
-
Potential of IDH mutations as immunotherapeutic targets in gliomas: a review and meta-analysis.Expert Opin Ther Targets. 2021 Dec;25(12):1045-1060. doi: 10.1080/14728222.2021.2017422. Expert Opin Ther Targets. 2021. PMID: 34904924 Review.
-
Advances in Immune Microenvironment and Immunotherapy of Isocitrate Dehydrogenase Mutated Glioma.Front Immunol. 2022 Jun 13;13:914618. doi: 10.3389/fimmu.2022.914618. eCollection 2022. Front Immunol. 2022. PMID: 35769466 Free PMC article. Review.
-
Immune microenvironment of gliomas.Lab Invest. 2017 May;97(5):498-518. doi: 10.1038/labinvest.2017.19. Epub 2017 Mar 13. Lab Invest. 2017. PMID: 28287634 Review.
-
Implications of IDH mutations on immunotherapeutic strategies for malignant glioma.Neurosurg Focus. 2022 Feb;52(2):E6. doi: 10.3171/2021.11.FOCUS21604. Neurosurg Focus. 2022. PMID: 35104795
-
Advances in the Immunotherapeutic Potential of Isocitrate Dehydrogenase Mutations in Glioma.Neurosci Bull. 2022 Sep;38(9):1069-1084. doi: 10.1007/s12264-022-00866-1. Epub 2022 Jun 7. Neurosci Bull. 2022. PMID: 35670952 Free PMC article. Review.
Cited by
-
Identification of Immune-Cell-Related Prognostic Biomarkers of Esophageal Squamous Cell Carcinoma Based on Tumor Microenvironment.Front Oncol. 2021 Oct 25;11:771749. doi: 10.3389/fonc.2021.771749. eCollection 2021. Front Oncol. 2021. PMID: 34760708 Free PMC article.
-
Non-cellular immunotherapies in pediatric central nervous system tumors.Front Immunol. 2023 Oct 11;14:1242911. doi: 10.3389/fimmu.2023.1242911. eCollection 2023. Front Immunol. 2023. PMID: 37885882 Free PMC article. Review.
-
The Immunomodulatory Effects of Fluorescein-Mediated Sonodynamic Treatment Lead to Systemic and Intratumoral Depletion of Myeloid-Derived Suppressor Cells in a Preclinical Malignant Glioma Model.Cancers (Basel). 2024 Feb 15;16(4):792. doi: 10.3390/cancers16040792. Cancers (Basel). 2024. PMID: 38398183 Free PMC article.
-
Epigenetic Suppression of the IL-7 Pathway in Progressive Glioblastoma.Biomedicines. 2022 Sep 2;10(9):2174. doi: 10.3390/biomedicines10092174. Biomedicines. 2022. PMID: 36140275 Free PMC article.
-
Emerging roles of ferroptosis in glioma.Front Oncol. 2022 Aug 22;12:993316. doi: 10.3389/fonc.2022.993316. eCollection 2022. Front Oncol. 2022. PMID: 36072803 Free PMC article. Review.
References
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
-
- Brat D.J., Aldape K., Colman H., Figrarella-Branger D., Fuller G.N., Giannini C., Holland E.C., Jenkins R.B., Kleinschmidt-DeMasters B., Komori T. cIMPACT-NOW update 5: Recommended grading criteria and terminologies for IDH-mutant astrocytomas. Acta Neuropathol. 2020;139:603–608. doi: 10.1007/s00401-020-02127-9. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
