

Immunology of Acute and Chronic Wound Healing
- PMID: 34066746
- PMCID: PMC8150999
- DOI: 10.3390/biom11050700
Immunology of Acute and Chronic Wound Healing
Abstract
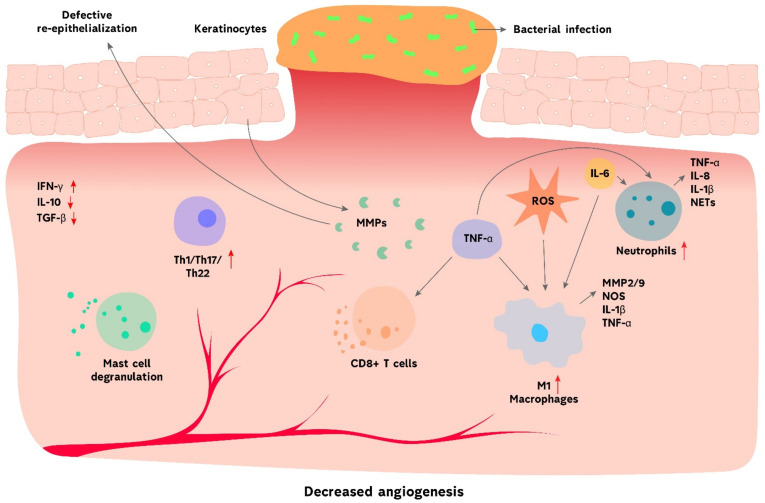
Skin wounds greatly affect the global healthcare system, creating a substantial burden on the economy and society. Moreover, the situation is exacerbated by low healing rates, which in fact are overestimated in reports. Cutaneous wounds are generally classified into acute and chronic. The immune response plays an important role during acute wound healing. The activation of immune cells and factors initiate the inflammatory process, facilitate wound cleansing and promote subsequent tissue healing. However, dysregulation of the immune system during the wound healing process leads to persistent inflammation and delayed healing, which ultimately result in chronic wounds. The microenvironment of a chronic wound is characterized by high quantities of pro-inflammatory macrophages, overexpression of inflammatory mediators such as TNF-α and IL-1β, increased activity of matrix metalloproteinases and abundance of reactive oxygen species. Moreover, chronic wounds are frequently complicated by bacterial biofilms, which perpetuate the inflammatory phase. Continuous inflammation and microbial biofilms make it very difficult for the chronic wounds to heal. In this review, we discuss the role of innate and adaptive immunity in the pathogenesis of acute and chronic wounds. Furthermore, we review the latest immunomodulatory therapeutic strategies, including modifying macrophage phenotype, regulating miRNA expression and targeting pro- and anti-inflammatory factors to improve wound healing.
Keywords: acute wound; adaptive immunity; chronic wound; cutaneous wound healing; innate immunity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Role of microRNA-21 and Its Underlying Mechanisms in Inflammatory Responses in Diabetic Wounds.Int J Mol Sci. 2020 May 8;21(9):3328. doi: 10.3390/ijms21093328. Int J Mol Sci. 2020. PMID: 32397166 Free PMC article.
-
Pseudomonas aeruginosa infection alters the macrophage phenotype switching process during wound healing in diabetic mice.Cell Biol Int. 2018 Jul;42(7):877-889. doi: 10.1002/cbin.10955. Epub 2018 Mar 14. Cell Biol Int. 2018. PMID: 29512223
-
Regulation of TH17 Cells and Associated Cytokines in Wound Healing, Tissue Regeneration, and Carcinogenesis.Int J Mol Sci. 2017 May 11;18(5):1033. doi: 10.3390/ijms18051033. Int J Mol Sci. 2017. PMID: 28492497 Free PMC article. Review.
-
NLRP3 activation induced by neutrophil extracellular traps sustains inflammatory response in the diabetic wound.Clin Sci (Lond). 2019 Feb 18;133(4):565-582. doi: 10.1042/CS20180600. Print 2019 Feb 28. Clin Sci (Lond). 2019. PMID: 30626731
-
Microenvironment and microbiology of skin wounds: the role of bacterial biofilms and related factors.Semin Vasc Surg. 2015 Sep-Dec;28(3-4):151-9. doi: 10.1053/j.semvascsurg.2016.01.003. Epub 2016 Jan 21. Semin Vasc Surg. 2015. PMID: 27113281 Review.
Cited by
-
Development of Biomaterials to Modulate the Function of Macrophages in Wound Healing.Bioengineering (Basel). 2024 Oct 12;11(10):1017. doi: 10.3390/bioengineering11101017. Bioengineering (Basel). 2024. PMID: 39451393 Free PMC article. Review.
-
Hybrid-Based Wound Dressings: Combination of Synthetic and Biopolymers.Polymers (Basel). 2022 Sep 12;14(18):3806. doi: 10.3390/polym14183806. Polymers (Basel). 2022. PMID: 36145951 Free PMC article. Review.
-
Pogostemon cablin Extract Promotes Wound Healing through OR2AT4 Activation and Exhibits Anti-Inflammatory Activity.Curr Issues Mol Biol. 2024 Aug 21;46(8):9136-9148. doi: 10.3390/cimb46080540. Curr Issues Mol Biol. 2024. PMID: 39194757 Free PMC article.
-
Therapeutic application of mesenchymal stem cell-derived exosomes in skin wound healing.Front Bioeng Biotechnol. 2024 Aug 5;12:1428793. doi: 10.3389/fbioe.2024.1428793. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 39161350 Free PMC article. Review.
-
Effect of Holoptelea integrifolia (Roxb.) Planch. n-Hexane Extract and Its Bioactive Compounds on Wound Healing and Anti-Inflammatory Activity.Molecules. 2022 Dec 4;27(23):8540. doi: 10.3390/molecules27238540. Molecules. 2022. PMID: 36500633 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
