

No Impact of Fluconazole to Echinocandins Replacement as First-Line Therapy on the Epidemiology of Yeast Fungemia (Hospital-Driven Active Surveillance, 2004-2017, Paris, France)
- PMID: 33959624
- PMCID: PMC8093410
- DOI: 10.3389/fmed.2021.641965
No Impact of Fluconazole to Echinocandins Replacement as First-Line Therapy on the Epidemiology of Yeast Fungemia (Hospital-Driven Active Surveillance, 2004-2017, Paris, France)
Abstract
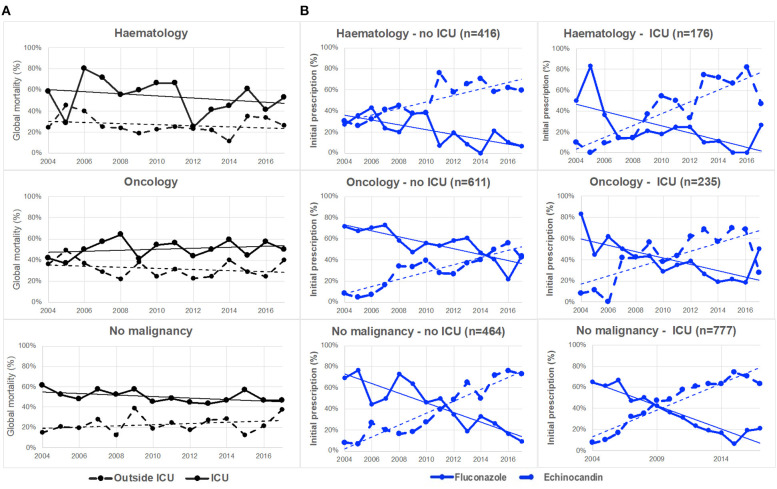
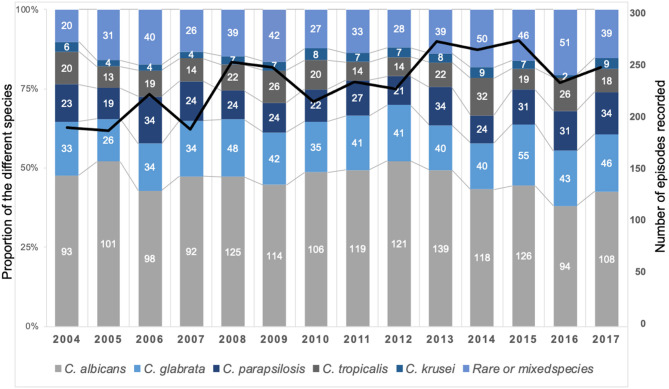
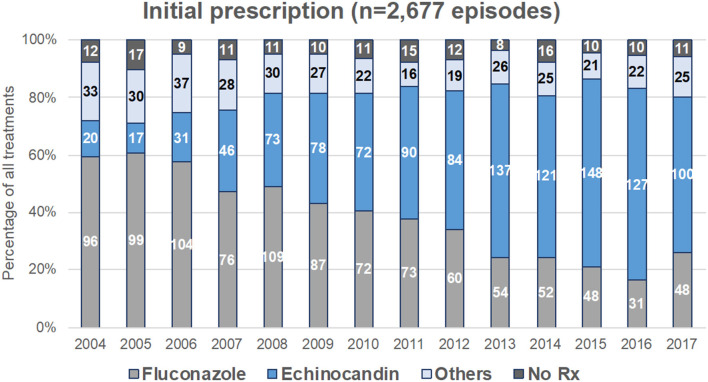
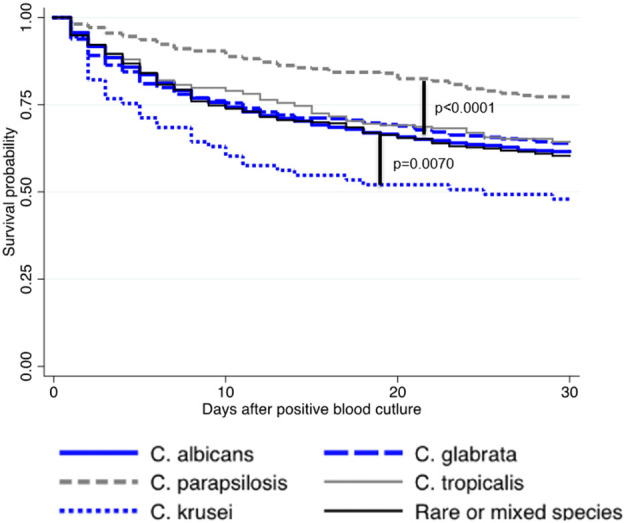
Replacement of fluconazole by echinocandins as the first-line therapy for yeast-related fungemia could have an impact on both the mortality rate and the epidemiology of yeast species responsible for candidemia. We analyzed the individual clinical and microbiological data collected through the active surveillance program on yeast fungemia (YEASTS program, 2004-2016, Paris area, France) within 14 University Hospitals. The cohort included 3,092 patients [male:female ratio: 1.56; median age 61.0 years (IQR: 23.8)]. The mean mortality rate within 30 days was 38.5% (1,103/2,868) and significantly higher in intensive care units (690/1,358, 50.8%) than outside (413/1,510, 27.4%, p < 0.0001) without significant change over time. The yeast species distribution [Candida albicans (n = 1,614, 48.0%), Candida glabrata (n = 607, 18.1%), Candida parapsilosis (n = 390, 11.6%), Candida tropicalis (n = 299, 8.9%), Candida krusei (n = 96, 2.9%), rare species (n = 357, 10.6%)], minimal inhibitory concentration distribution, and the distribution between the patient populations (hematological malignancies, solid tumors, without malignancy) did not change either while the proportion of patients ≥60-years increased from 48.7% (91/187) in 2004 to 56.8% (133/234) in 2017 (p = 0.0002). Fluconazole as first-line therapy dramatically decreased (64.4% in 2004 to 27.7% in 2017, p < 0.0001) with a corresponding increase in echinocandins (11.6% in 2004 to 57.8% in 2017, p < 0.0001). Survival rates did not differ according to the first antifungal therapy. The progressive replacement of fluconazole by echinocandins as the first-line antifungal therapy was not associated with change in global mortality, regardless of species involved and antifungal susceptibility profiles. Other factors remain to be uncovered to improve the prognosis of yeast fungemia.
Keywords: candidemia; echinocandins; epidemiology; fluconazole; fungemia; hematological malignancy; intensive care unit; solid cancer.
Copyright © 2021 Bretagne, Desnos-Ollivier, Sitbon, Lortholary, Che, Dromer and Participants of the YEASTS.
Conflict of interest statement
SB has received travel grant from Pfizer in 2018 and has served on scientific advisory board for Gilead until 2018. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Candida and candidaemia. Susceptibility and epidemiology.Dan Med J. 2013 Nov;60(11):B4698. Dan Med J. 2013. PMID: 24192246 Review.
-
The risk and clinical outcome of candidemia depending on underlying malignancy.Intensive Care Med. 2017 May;43(5):652-662. doi: 10.1007/s00134-017-4743-y. Epub 2017 Mar 20. Intensive Care Med. 2017. PMID: 28321466 Free PMC article.
-
Antifungal susceptibility of Candida species isolated from patients with candidemia in southern Taiwan, 2007-2012: impact of new antifungal breakpoints.Mycoses. 2017 Feb;60(2):89-95. doi: 10.1111/myc.12553. Epub 2016 Sep 12. Mycoses. 2017. PMID: 27621210
-
Population-Based Active Surveillance for Culture-Confirmed Candidemia - Four Sites, United States, 2012-2016.MMWR Surveill Summ. 2019 Sep 27;68(8):1-15. doi: 10.15585/mmwr.ss6808a1. MMWR Surveill Summ. 2019. PMID: 31557145 Free PMC article.
-
Mixed fungaemia: an 18-year report from a tertiary-care university hospital and a systematic review.Clin Microbiol Infect. 2020 Jul;26(7):833-841. doi: 10.1016/j.cmi.2020.03.030. Epub 2020 Apr 1. Clin Microbiol Infect. 2020. PMID: 32246995 Review.
Cited by
-
In Vivo Efficacy of Rezafungin, Anidulafungin, Caspofungin, and Micafungin against Four Candida auris Clades in a Neutropenic Mouse Bloodstream Infection Model.J Fungi (Basel). 2024 Aug 29;10(9):617. doi: 10.3390/jof10090617. J Fungi (Basel). 2024. PMID: 39330378 Free PMC article.
-
Echinocandins Susceptibility Patterns of 2,787 Yeast Isolates: Importance of the Thresholds for the Detection of FKS Mutations.Antimicrob Agents Chemother. 2022 May 17;66(5):e0172521. doi: 10.1128/aac.01725-21. Epub 2022 Apr 12. Antimicrob Agents Chemother. 2022. PMID: 35412354 Free PMC article.
-
COVID-19-Associated Pulmonary Aspergillosis, Fungemia, and Pneumocystosis in the Intensive Care Unit: a Retrospective Multicenter Observational Cohort during the First French Pandemic Wave.Microbiol Spectr. 2021 Oct 31;9(2):e0113821. doi: 10.1128/Spectrum.01138-21. Epub 2021 Oct 20. Microbiol Spectr. 2021. PMID: 34668768 Free PMC article.
-
Active Surveillance Program to Increase Awareness on Invasive Fungal Diseases: the French RESSIF Network (2012 to 2018).mBio. 2022 Jun 28;13(3):e0092022. doi: 10.1128/mbio.00920-22. Epub 2022 May 2. mBio. 2022. PMID: 35499498 Free PMC article.
-
Candida haemulonii complex, an emerging threat from tropical regions?PLoS Negl Trop Dis. 2023 Jul 31;17(7):e0011453. doi: 10.1371/journal.pntd.0011453. eCollection 2023 Jul. PLoS Negl Trop Dis. 2023. PMID: 37523406 Free PMC article. Review.
References
-
- Colombo AL, Guimarães T, Camargo LFA, Richtmann R, Queiroz-Telles F, de Salles MJC, et al. . Brazilian guidelines for the management of candidiasis—a joint meeting report of three medical societies: sociedade Brasileira de Infectologia, Sociedade Paulista de Infectologia and Sociedade Brasileira de Medicina Tropical. Braz J Infect Dis. (2013) 17:283–312. 10.1016/j.bjid.2013.02.001 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources