

Gastrointestinal mucosal damage in patients with COVID-19 undergoing endoscopy: an international multicentre study
- PMID: 33627313
- PMCID: PMC7907837
- DOI: 10.1136/bmjgast-2020-000578
Gastrointestinal mucosal damage in patients with COVID-19 undergoing endoscopy: an international multicentre study
Abstract
Background: Although evidence suggests frequent gastrointestinal (GI) involvement during coronavirus disease 2019 (COVID-19), endoscopic findings are scarcely reported.
Aims: We aimed at registering endoscopic abnormalities and potentially associated risk factors among patients with COVID-19.
Methods: All consecutive patients with COVID-19 undergoing endoscopy in 16 institutions from high-prevalence regions were enrolled. Mann-Whitney U, χ2 or Fisher's exact test were used to compare patients with major abnormalities to those with negative procedures, and multivariate logistic regression to identify independent predictors.
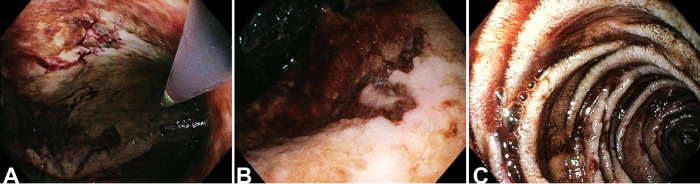
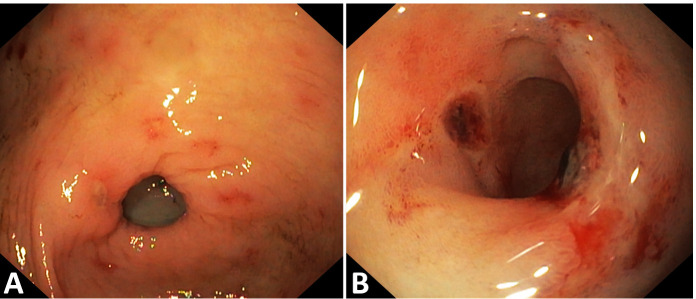
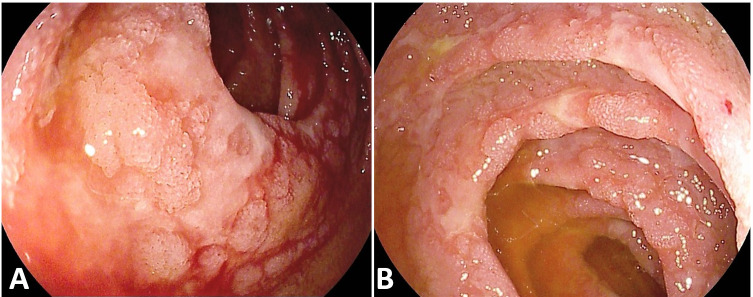
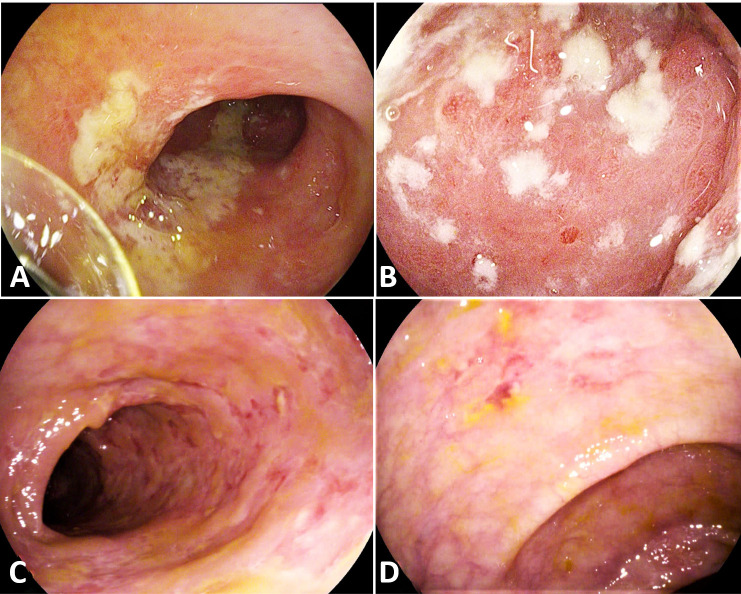
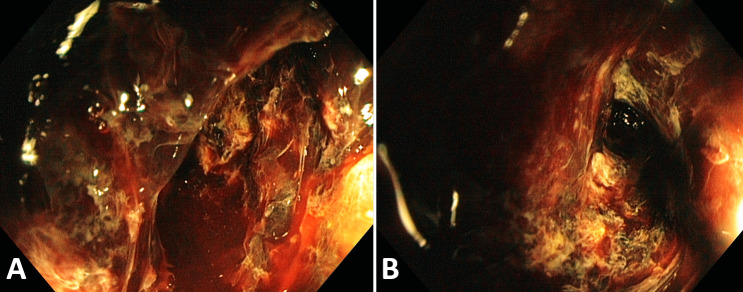
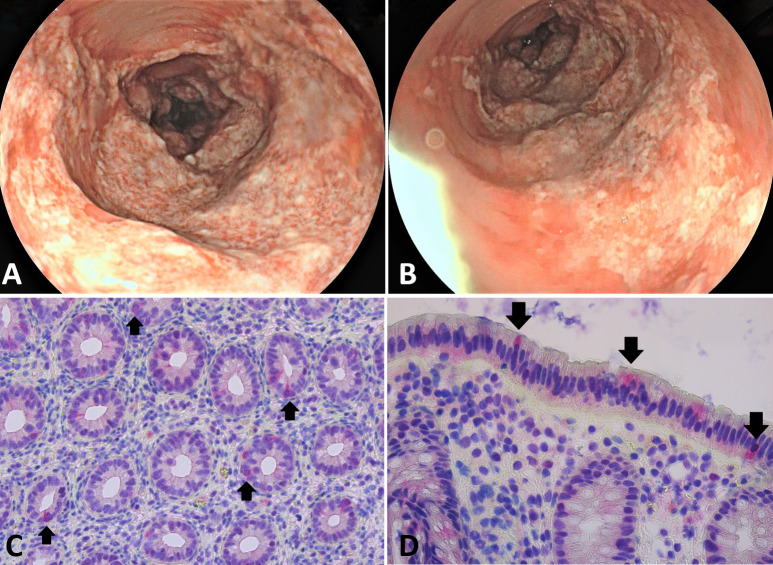
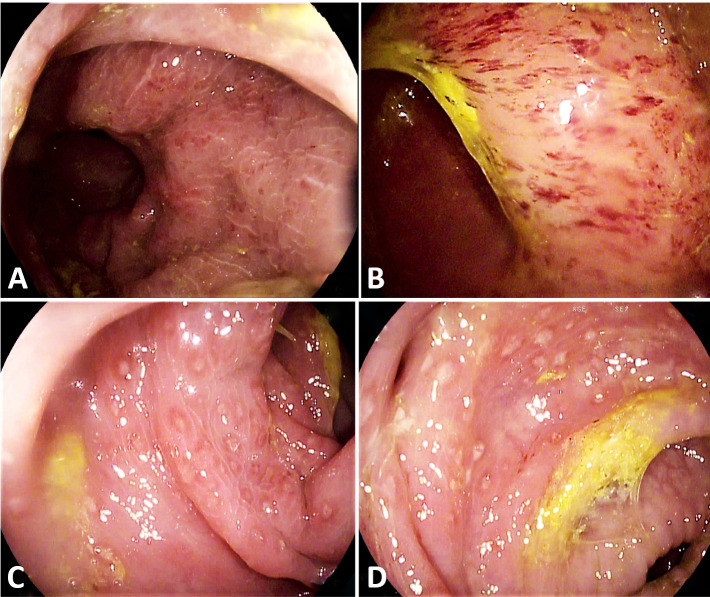
Results: Between February and May 2020, during the first pandemic outbreak with severely restricted endoscopy activity, 114 endoscopies on 106 patients with COVID-19 were performed in 16 institutions (men=70.8%, median age=68 (58-74); 33% admitted in intensive care unit; 44.4% reporting GI symptoms). 66.7% endoscopies were urgent, mainly for overt GI bleeding. 52 (45.6%) patients had major abnormalities, whereas 13 bled from previous conditions. The most prevalent upper GI abnormalities were ulcers (25.3%), erosive/ulcerative gastro-duodenopathy (16.1%) and petechial/haemorrhagic gastropathy (9.2%). Among lower GI endoscopies, 33.3% showed an ischaemic-like colitis.Receiver operating curve analysis identified D-dimers >1850 ng/mL as predicting major abnormalities. Only D-dimers >1850 ng/mL (OR=12.12 (1.69-86.87)) and presence of GI symptoms (OR=6.17 (1.13-33.67)) were independently associated with major abnormalities at multivariate analysis.
Conclusion: In this highly selected cohort of hospitalised patients with COVID-19 requiring endoscopy, almost half showed acute mucosal injuries and more than one-third of lower GI endoscopies had features of ischaemic colitis. Among the hospitalisation-related and patient-related variables evaluated in this study, D-dimers above 1850 ng/mL was the most useful at predicting major mucosal abnormalities at endoscopy.
Trial registration number: ClinicalTrial.gov (ID: NCT04318366).
Keywords: covid-19; endoscopy; gastrointestinal tract; mucosal infection.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GV received travel grants from Mylan and Alfasigma. GC is a consultant for Mylan. IB is consultant for Apollo Endosurgery, Cook Medical and Boston Scientific; board member for Endo Tools; research grant recipient from Apollo Endosurgery; had food and beverage compensation from Apollo Endosurgery, Cook Medical, Boston Scientific and Endo Tools. LR is a consultant for Cancer Prevention Pharmaceuticals; has received research grants from SLA Pharma AG and Takeda and receives funds from the Italian Association for Cancer Research (IG21723). MB received travel grants from Takeda, Taewoong Medical and Prion Medical. KWO has received lecture fees from Olympus, Medtronic and Mylan. He has received a research grant from Medtronic. LP received advisory board fees from Janssen and Takeda; presentation fees from AbbVie and Ferring; and personal fees from AbbVie, Ferring, Norgine and Takeda. SWVdM holds the Cook chair in interventional endoscopy and holds consultancy agreements with Boston Scientific, Cook, Pentax and Olympus. ES has received lecture or consultancy fees from Medtronic, Reckitt Benckiser, Takeda, Merck & Co, Bristol Myers Squibb, AbbVie, Amgen, Novartis, Fresenius Kabi, Sandoz, Sofar, Malesci, Janssen, Grifols, Aurora Pharma, Innovamedica, Johnson & Johnson, SILA, Unifarco, Alfasigma, Shire, EG Stada Group. MK has done consulting work for Boston Scientific, Interscope Med and AbbVie. He has received research grants from Boston Scientific, Emcision, Conmed, Pinnacle, Cook, Gore, Merit and Olympus. PR is supported by Clinical Mandate from Belgian Foundation against Cancer (Stichting tegen Kanker) and receives speaking and consultancy fees from MSD Belgium. GC is consultant for and had food and beverage compensation from Cook Medical, Boston Scientific and Olympus.
Figures
Similar articles
-
COVID-19 AND DIGESTIVE ENDOSCOPY: EMERGENCY ENDOSCOPIC PROCEDURES AND RISK FACTORS FOR UPPER GASTROINTESTINAL BLEEDING.Arq Gastroenterol. 2021 Jul-Sep;58(3):337-343. doi: 10.1590/S0004-2803.202100000-57. Arq Gastroenterol. 2021. PMID: 34705968
-
[Acute hemorrhage of the upper part of the gastrointestinal tract--survey of emergency endoscopy of the upper gastrointestinal tract at our facility].Vnitr Lek. 2004 Apr;50(4):274-7. Vnitr Lek. 2004. PMID: 15214296 Czech.
-
A Questionnaire-Based Survey on the Impact of the COVID-19 Pandemic on Gastrointestinal Endoscopy in Asia.Digestion. 2022;103(1):7-21. doi: 10.1159/000520287. Epub 2021 Nov 10. Digestion. 2022. PMID: 34758472 Free PMC article.
-
Gastrointestinal Bleeding in COVID-19-Infected Patients.Gastroenterol Clin North Am. 2023 Mar;52(1):77-102. doi: 10.1016/j.gtc.2022.10.004. Epub 2022 Nov 1. Gastroenterol Clin North Am. 2023. PMID: 36813432 Free PMC article. Review.
-
COVID-19 and gastrointestinal endoscopies: Current insights and emergent strategies.Dig Endosc. 2020 Jul;32(5):715-722. doi: 10.1111/den.13693. Epub 2020 Jun 3. Dig Endosc. 2020. PMID: 32281689 Free PMC article. Review.
Cited by
-
A case of COVID-19 diarrhea relieved by bile acid sequestrant administration.Clin J Gastroenterol. 2022 Apr;15(2):393-400. doi: 10.1007/s12328-022-01598-5. Epub 2022 Feb 4. Clin J Gastroenterol. 2022. PMID: 35122223 Free PMC article.
-
Neutrophil Activation and Immune Thrombosis Profiles Persist in Convalescent COVID-19.J Clin Immunol. 2023 Jul;43(5):882-893. doi: 10.1007/s10875-023-01459-x. Epub 2023 Mar 21. J Clin Immunol. 2023. PMID: 36943669 Free PMC article.
-
Excess Deaths of Gastrointestinal, Liver, and Pancreatic Diseases During the COVID-19 Pandemic in the United States.Int J Public Health. 2023 Aug 15;68:1606305. doi: 10.3389/ijph.2023.1606305. eCollection 2023. Int J Public Health. 2023. PMID: 37649691 Free PMC article.
-
Incidence of persistent SARS-CoV-2 gut infection in patients with a history of COVID-19: Insights from endoscopic examination.Endosc Int Open. 2024 Jan 5;12(1):E11-E22. doi: 10.1055/a-2180-9872. eCollection 2024 Jan. Endosc Int Open. 2024. PMID: 38188925 Free PMC article.
-
COVID-19 and Gastrointestinal Tract: From Pathophysiology to Clinical Manifestations.Medicina (Kaunas). 2023 Sep 24;59(10):1709. doi: 10.3390/medicina59101709. Medicina (Kaunas). 2023. PMID: 37893427 Free PMC article. Review.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical