

Dysnatremia is a Predictor for Morbidity and Mortality in Hospitalized Patients with COVID-19
- PMID: 33624101
- PMCID: PMC7928894
- DOI: 10.1210/clinem/dgab107
Dysnatremia is a Predictor for Morbidity and Mortality in Hospitalized Patients with COVID-19
Abstract
Context: Dysnatremia is an independent predictor of mortality in patients with bacterial pneumonia. There is paucity of data about the incidence and prognostic impact of abnormal sodium concentration in patients with coronavirus disease 2019 (COVID-19).
Objective: This work aimed to examine the association of serum sodium during hospitalization with key clinical outcomes, including mortality, need for advanced respiratory support and acute kidney injury (AKI), and to explore the role of serum sodium as a marker of inflammatory response in COVID-19.
Methods: This retrospective longitudinal cohort study, including all adult patients who presented with COVID-19 to 2 hospitals in London over an 8-week period, evaluated the association of dysnatremia (serum sodium < 135 or > 145 mmol/L, hyponatremia, and hypernatremia, respectively) at several time points with inpatient mortality, need for advanced ventilatory support, and AKI.
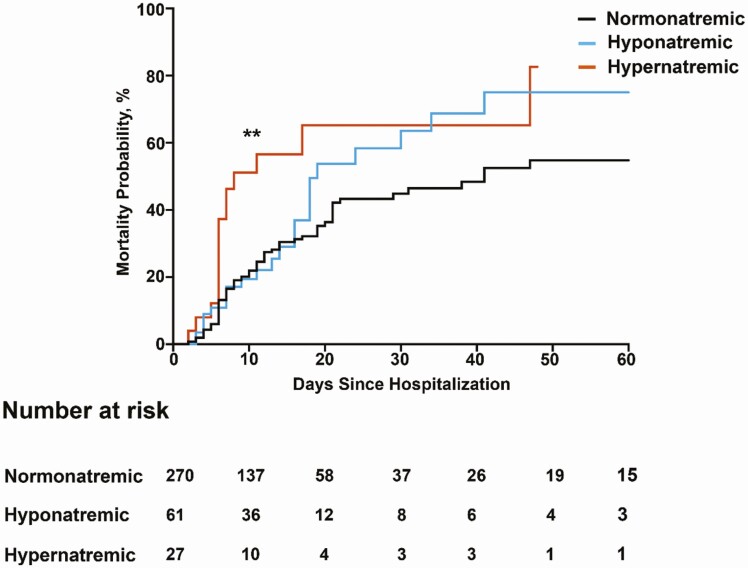
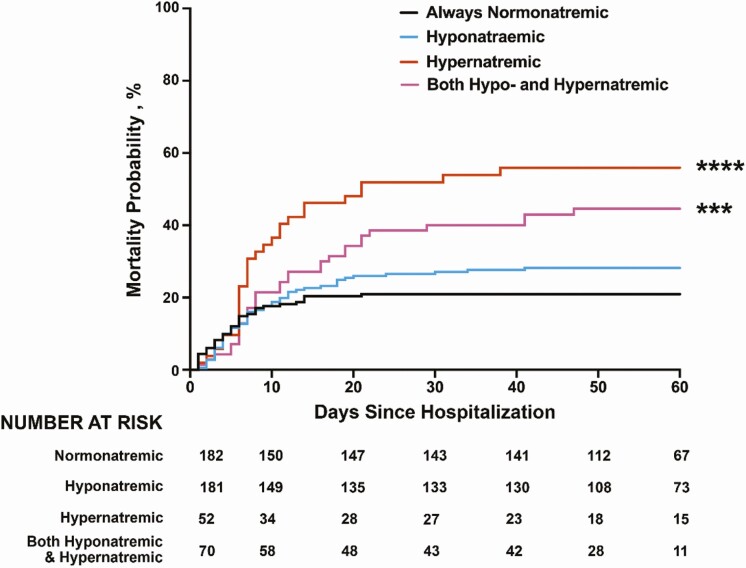
Results: The study included 488 patients (median age, 68 years). At presentation, 24.6% of patients were hyponatremic, mainly due to hypovolemia, and 5.3% hypernatremic. Hypernatremia 2 days after admission and exposure to hypernatremia at any time point during hospitalization were associated with a 2.34-fold (95% CI, 1.08-5.05; P = .0014) and 3.05-fold (95% CI, 1.69-5.49; P < .0001) increased risk of death, respectively, compared to normonatremia. Hyponatremia at admission was linked with a 2.18-fold increase in the likelihood of needing ventilatory support (95% CI, 1.34-3.45, P = .0011). Hyponatremia was not a risk factor for in-hospital mortality, except for the subgroup of patients with hypovolemic hyponatremia. Sodium values were not associated with the risk for AKI and length of hospital stay.
Conclusion: Abnormal sodium levels during hospitalization are risk factors for poor prognosis, with hypernatremia and hyponatremia being associated with a greater risk of death and respiratory failure, respectively. Serum sodium values could be used for risk stratification in patients with COVID-19.
Keywords: COVID-19; SARS-CoV-2; SIAD; hypernatremia; hyponatremia; sodium.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Electrolytes and COVID-19: challenges and caveats in clinical research studies.J Nephrol. 2023 Apr;36(3):929-931. doi: 10.1007/s40620-022-01434-6. Epub 2022 Aug 18. J Nephrol. 2023. PMID: 35980534 Free PMC article. No abstract available.
Similar articles
-
Prognostic Impact of Hyponatremia and Hypernatremia in COVID-19 Pneumonia. A HOPE-COVID-19 (Health Outcome Predictive Evaluation for COVID-19) Registry Analysis.Front Endocrinol (Lausanne). 2020 Nov 30;11:599255. doi: 10.3389/fendo.2020.599255. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33329400 Free PMC article.
-
Serum sodium alterations in SARS CoV-2 (COVID-19) infection: impact on patient outcome.Eur J Endocrinol. 2021 May 28;185(1):137-144. doi: 10.1530/EJE-20-1447. Eur J Endocrinol. 2021. PMID: 33950864 Free PMC article.
-
Dysnatremia is an Independent Indicator of Mortality in Hospitalized Patients.Med Sci Monit. 2017 May 21;23:2408-2425. doi: 10.12659/msm.902032. Med Sci Monit. 2017. PMID: 28528344 Free PMC article.
-
Acute Dysnatremias - a dangerous and overlooked clinical problem.Scand J Trauma Resusc Emerg Med. 2019 May 28;27(1):58. doi: 10.1186/s13049-019-0633-3. Scand J Trauma Resusc Emerg Med. 2019. PMID: 31138251 Free PMC article. Review.
-
Preventing neurological complications from dysnatremias in children.Pediatr Nephrol. 2005 Dec;20(12):1687-700. doi: 10.1007/s00467-005-1933-6. Epub 2005 Aug 4. Pediatr Nephrol. 2005. PMID: 16079988 Review.
Cited by
-
Hyponatremia after COVID-19 is frequent in the first year and increases re-admissions.Sci Rep. 2024 Jan 5;14(1):595. doi: 10.1038/s41598-023-50970-z. Sci Rep. 2024. PMID: 38182711 Free PMC article.
-
The Mutual Relationship among Cardiovascular Diseases and COVID-19: Focus on Micronutrients Imbalance.Nutrients. 2022 Aug 21;14(16):3439. doi: 10.3390/nu14163439. Nutrients. 2022. PMID: 36014944 Free PMC article. Review.
-
Syndrome of inappropriate antidiuresis/hyponatremia in COVID-19.Pituitary. 2024 Dec;27(6):889-897. doi: 10.1007/s11102-024-01446-4. Epub 2024 Aug 28. Pituitary. 2024. PMID: 39196447 Free PMC article. Review.
-
[Dysnatremias and their association with morbidity and mortality in patients with COVID- 19].Rev Med Inst Mex Seguro Soc. 2022 Aug 31;60(5):548-555. Rev Med Inst Mex Seguro Soc. 2022. PMID: 36048807 Free PMC article. Spanish.
-
The impact of the correction of hyponatremia during hospital admission on the prognosis of SARS-CoV-2 infection.Med Clin (Engl Ed). 2022 Jul 8;159(1):12-18. doi: 10.1016/j.medcle.2021.07.021. Epub 2022 Jun 29. Med Clin (Engl Ed). 2022. PMID: 35784827 Free PMC article.
References
-
- Levy TJ, Richardson S, Coppa K, et al. . Development and validation of a survival calculator for hospitalized patients with COVID-19. medRxiv. doi:10.1101/2020.04.22.20075416, June 2, 2020, preprint: not peer reviewed.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
