

Impact of the COVID-19 pandemic on faecal immunochemical test-based colorectal cancer screening programmes in Australia, Canada, and the Netherlands: a comparative modelling study
- PMID: 33548185
- PMCID: PMC9767453
- DOI: 10.1016/S2468-1253(21)00003-0
Impact of the COVID-19 pandemic on faecal immunochemical test-based colorectal cancer screening programmes in Australia, Canada, and the Netherlands: a comparative modelling study
Abstract
Background: Colorectal cancer screening programmes worldwide have been disrupted during the COVID-19 pandemic. We aimed to estimate the impact of hypothetical disruptions to organised faecal immunochemical test-based colorectal cancer screening programmes on short-term and long-term colorectal cancer incidence and mortality in three countries using microsimulation modelling.
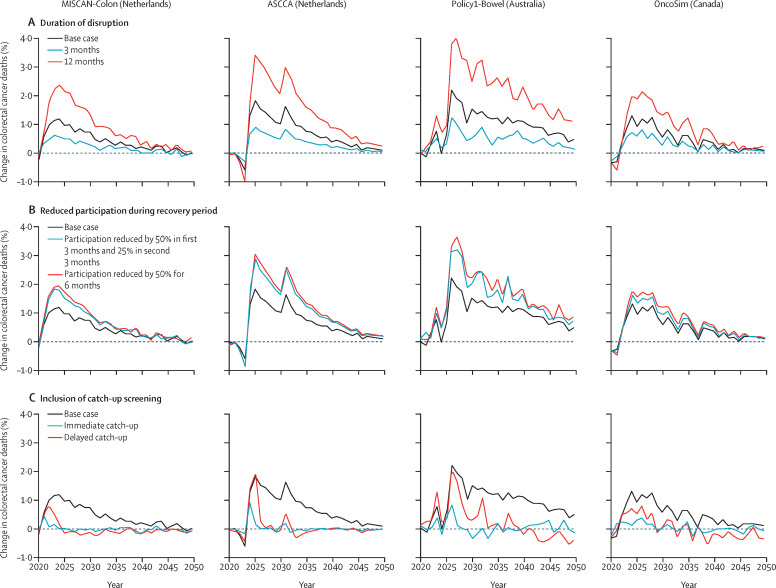
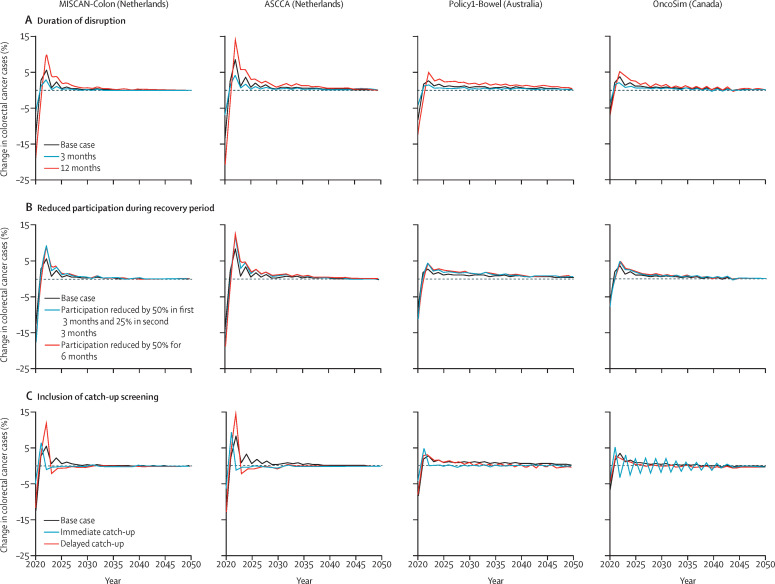
Methods: In this modelling study, we used four country-specific colorectal cancer microsimulation models-Policy1-Bowel (Australia), OncoSim (Canada), and ASCCA and MISCAN-Colon (the Netherlands)-to estimate the potential impact of COVID-19-related disruptions to screening on colorectal cancer incidence and mortality in Australia, Canada, and the Netherlands annually for the period 2020-24 and cumulatively for the period 2020-50. Modelled scenarios varied by duration of disruption (3, 6, and 12 months), decreases in screening participation after the period of disruption (0%, 25%, or 50% reduction), and catch-up screening strategies (within 6 months after the disruption period or all screening delayed by 6 months).
Findings: Without catch-up screening, our analysis predicted that colorectal cancer deaths among individuals aged 50 years and older, a 3-month disruption would result in 414-902 additional new colorectal cancer diagnoses (relative increase 0·1-0·2%) and 324-440 additional deaths (relative increase 0·2-0·3%) in the Netherlands, 1672 additional diagnoses (relative increase 0·3%) and 979 additional deaths (relative increase 0·5%) in Australia, and 1671 additional diagnoses (relative increase 0·2%) and 799 additional deaths (relative increase 0·3%) in Canada between 2020 and 2050, compared with undisrupted screening. A 6-month disruption would result in 803-1803 additional diagnoses (relative increase 0·2-0·4%) and 678-881 additional deaths (relative increase 0·4-0·6%) in the Netherlands, 3552 additional diagnoses (relative increase 0·6%) and 1961 additional deaths (relative increase 1·0%) in Australia, and 2844 additional diagnoses (relative increase 0·3%) and 1319 additional deaths (relative increase 0·4%) in Canada between 2020 and 2050, compared with undisrupted screening. A 12-month disruption would result in 1619-3615 additional diagnoses (relative increase 0·4-0·9%) and 1360-1762 additional deaths (relative increase 0·8-1·2%) in the Netherlands, 7140 additional diagnoses (relative increase 1·2%) and 3968 additional deaths (relative increase 2·0%) in Australia, and 5212 additional diagnoses (relative increase 0·6%) and 2366 additional deaths (relative increase 0·8%) in Canada between 2020 and 2050, compared with undisrupted screening. Providing immediate catch-up screening could minimise the impact of the disruption, restricting the relative increase in colorectal cancer incidence and deaths between 2020 and 2050 to less than 0·1% in all countries. A post-disruption decrease in participation could increase colorectal cancer incidence by 0·2-0·9% and deaths by 0·6-1·6% between 2020 and 2050, compared with undisrupted screening.
Interpretation: Although the projected effect of short-term disruption to colorectal cancer screening is modest, such disruption will have a marked impact on colorectal cancer incidence and deaths between 2020 and 2050 attributable to missed screening. Thus, it is crucial that, if disrupted, screening programmes ensure participation rates return to previously observed rates and provide catch-up screening wherever possible, since this could mitigate the impact on colorectal cancer deaths.
Funding: Cancer Council New South Wales, Health Canada, and Dutch National Institute for Public Health and Environment.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Impairment of colorectal cancer screening during the COVID-19 pandemic.Lancet Gastroenterol Hepatol. 2021 Jun;6(6):425-426. doi: 10.1016/S2468-1253(21)00098-4. Lancet Gastroenterol Hepatol. 2021. PMID: 34015352 Free PMC article. No abstract available.
-
Impairment of colorectal cancer screening during the COVID-19 pandemic.Lancet Gastroenterol Hepatol. 2021 Jun;6(6):426. doi: 10.1016/S2468-1253(21)00136-9. Lancet Gastroenterol Hepatol. 2021. PMID: 34015353 Free PMC article. No abstract available.
Similar articles
-
Prioritisation of colonoscopy services in colorectal cancer screening programmes to minimise impact of COVID-19 pandemic on predicted cancer burden: A comparative modelling study.J Med Screen. 2022 Jun;29(2):72-83. doi: 10.1177/09691413211056777. Epub 2021 Dec 3. J Med Screen. 2022. PMID: 35100894 Free PMC article.
-
Potential global loss of life expected due to COVID-19 disruptions to organised colorectal cancer screening.EClinicalMedicine. 2023 Jul 20;62:102081. doi: 10.1016/j.eclinm.2023.102081. eCollection 2023 Aug. EClinicalMedicine. 2023. PMID: 37538541 Free PMC article.
-
COVID-related disruptions to colorectal cancer screening, diagnosis, and treatment could increase cancer Burden in Australia and Canada: A modelling study.PLoS One. 2024 Apr 1;19(4):e0296945. doi: 10.1371/journal.pone.0296945. eCollection 2024. PLoS One. 2024. PMID: 38557758 Free PMC article.
-
Current international developments in population screening for colorectal cancer.ANZ J Surg. 2002 Jul;72(7):507-12. doi: 10.1046/j.1445-2197.2002.02472.x. ANZ J Surg. 2002. PMID: 12123514 Review.
-
Screening for colorectal cancer using the faecal occult blood test, Hemoccult.Cochrane Database Syst Rev. 2007 Jan 24;2007(1):CD001216. doi: 10.1002/14651858.CD001216.pub2. Cochrane Database Syst Rev. 2007. PMID: 17253456 Free PMC article. Review.
Cited by
-
Israeli COVID lockdowns mildly reduced overall use of preventive health services, but exacerbated some disparities.Int J Qual Health Care. 2022 Sep 16;34(3):mzac071. doi: 10.1093/intqhc/mzac071. Int J Qual Health Care. 2022. PMID: 36062971 Free PMC article.
-
Prevention and screening during the COVID-19 pandemic: qualitative findings from the BETTER WISE project.BMC Prim Care. 2023 Jan 23;24(1):27. doi: 10.1186/s12875-022-01954-x. BMC Prim Care. 2023. PMID: 36690937 Free PMC article.
-
Systematic review: non-endoscopic surveillance for colorectal neoplasia in individuals with Lynch syndrome.Aliment Pharmacol Ther. 2022 Apr;55(7):778-788. doi: 10.1111/apt.16824. Epub 2022 Feb 18. Aliment Pharmacol Ther. 2022. PMID: 35181895 Free PMC article.
-
Modelling optimal use of temporarily restricted colonoscopy capacity in a FIT-based CRC screening program: Application during the COVID-19 pandemic.PLoS One. 2022 Jun 24;17(6):e0270223. doi: 10.1371/journal.pone.0270223. eCollection 2022. PLoS One. 2022. PMID: 35749423 Free PMC article.
-
Impact of the COVID-19 pandemic on the management of colorectal cancer in Denmark.BJS Open. 2021 Nov 9;5(6):zrab108. doi: 10.1093/bjsopen/zrab108. BJS Open. 2021. PMID: 34755189 Free PMC article.
References
-
- WHO WHO coronavirus disease (COVID-19) dashboard. https://covid19.who.int/
-
- International Agency for Research on Cancer . International Agency for Research on Cancer; Lyon: 2017. IARC Handbooks of Cancer Prevention: colorectal cancer screening.
-
- Van den Brink C, Van den Ende C, Eeuwijk J, et al. National Institute for Public Health and Environment; Bilthoven: 2020. Kort-cyclische rapportage indirecte effecten COVID-19 op zorg en gezondheid.
-
- Lee J. CBC Canada; Toronto, ON: May 27, 2020. Thousands of cancer screening tests halted during pandemic restart in Alberta.https://www.cbc.ca/news/canada/calgary/alberta-cancer-screening-resumes-...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
