

Prosociality predicts health behaviors during the COVID-19 pandemic
- PMID: 33531719
- PMCID: PMC7842154
- DOI: 10.1016/j.jpubeco.2021.104367
Prosociality predicts health behaviors during the COVID-19 pandemic
Abstract
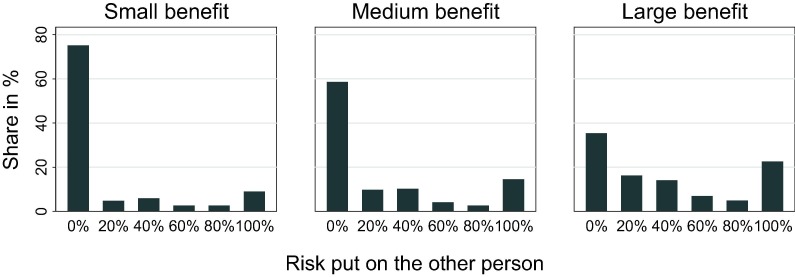
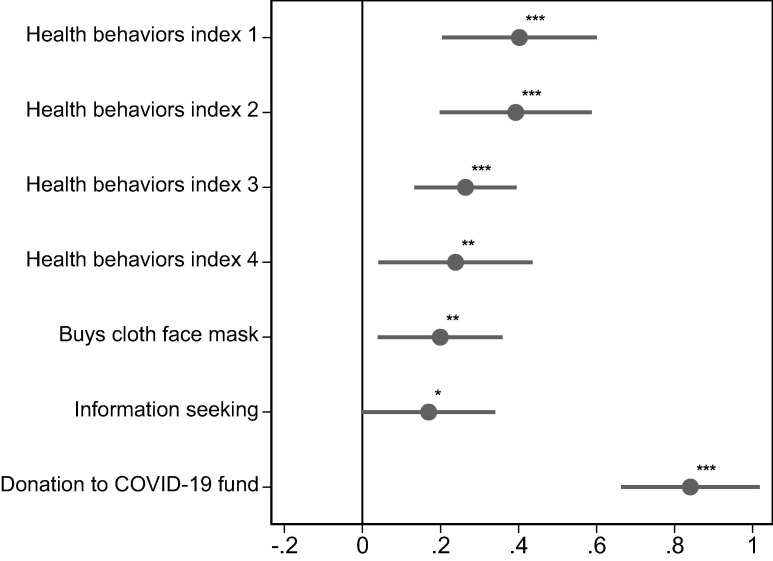
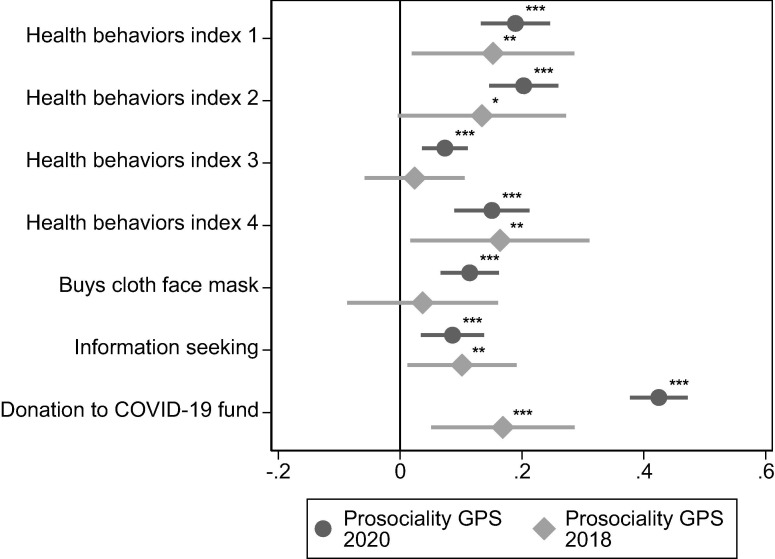
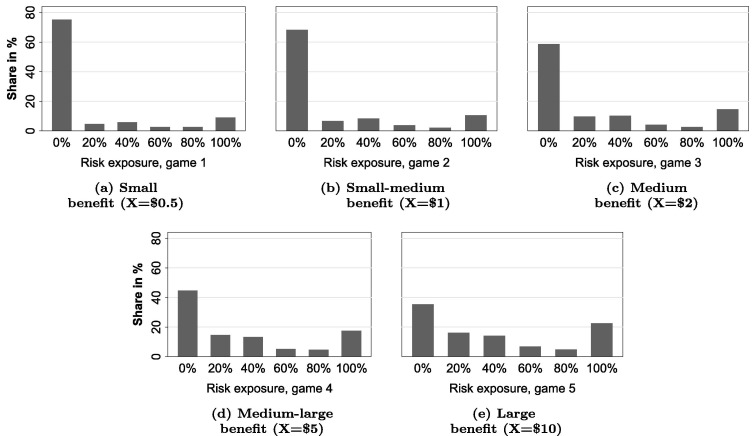
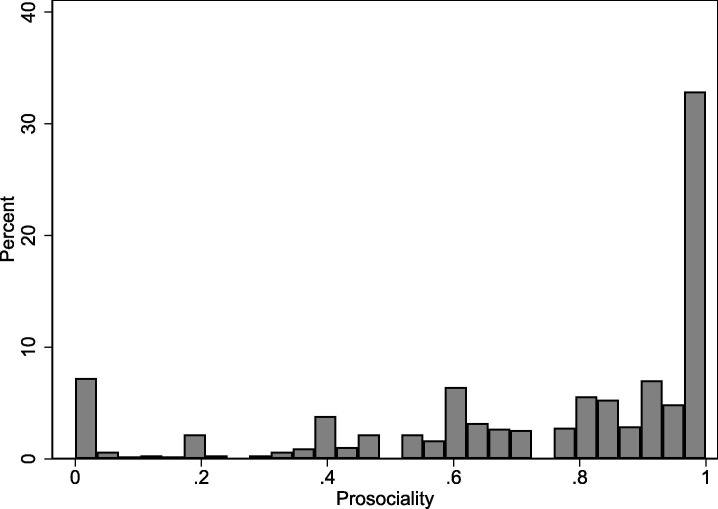
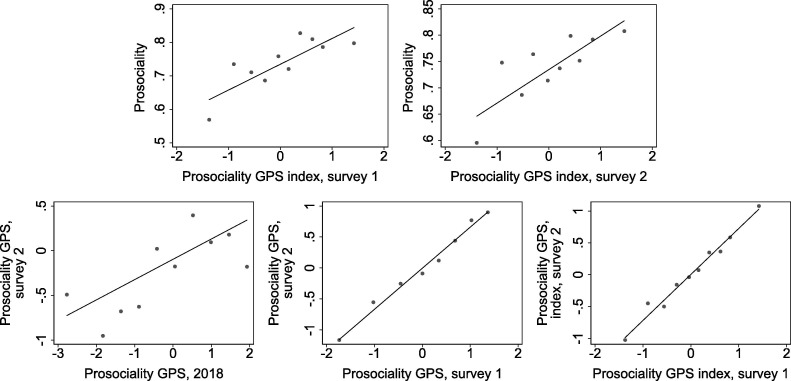
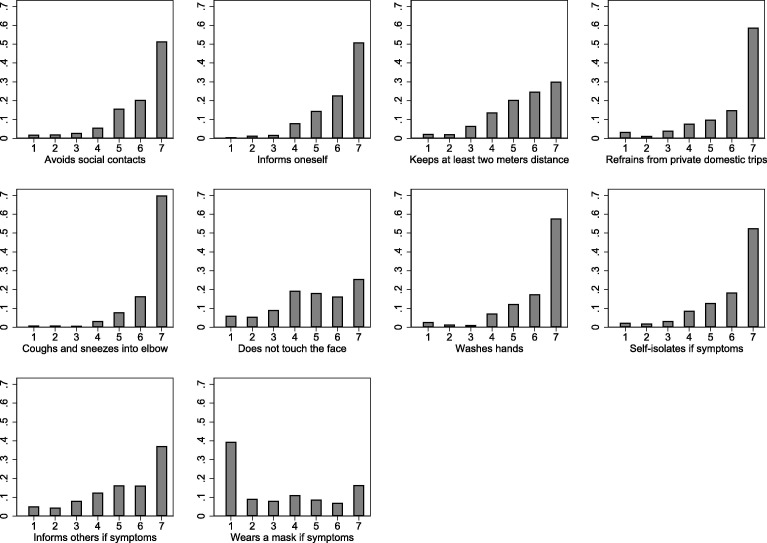
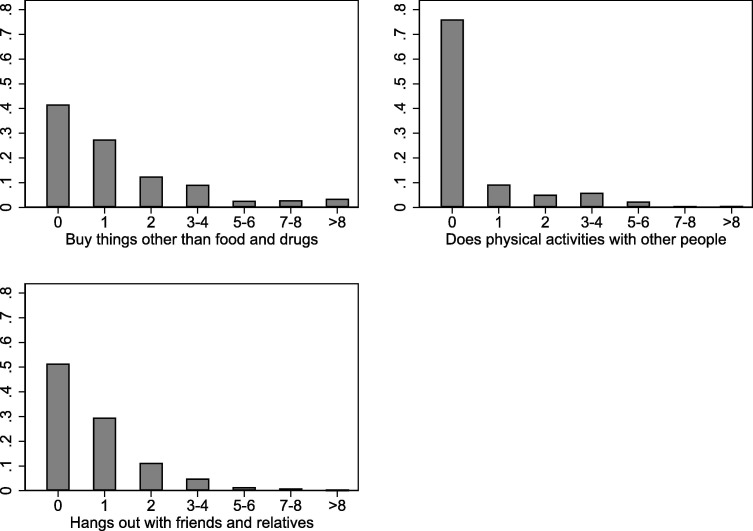
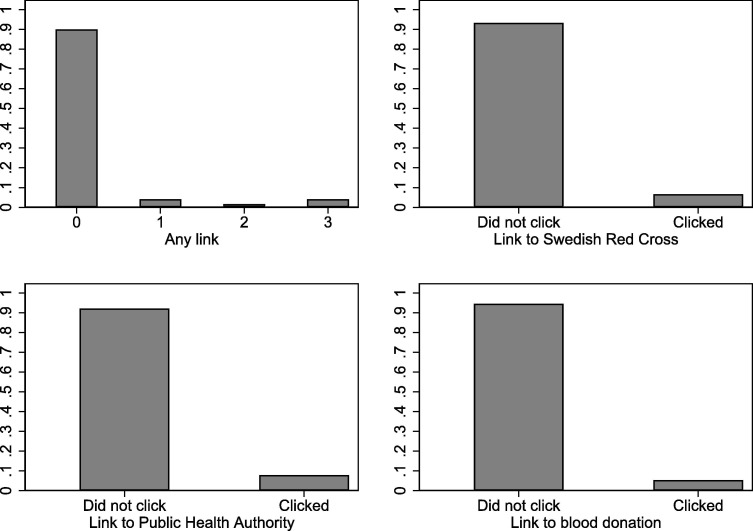
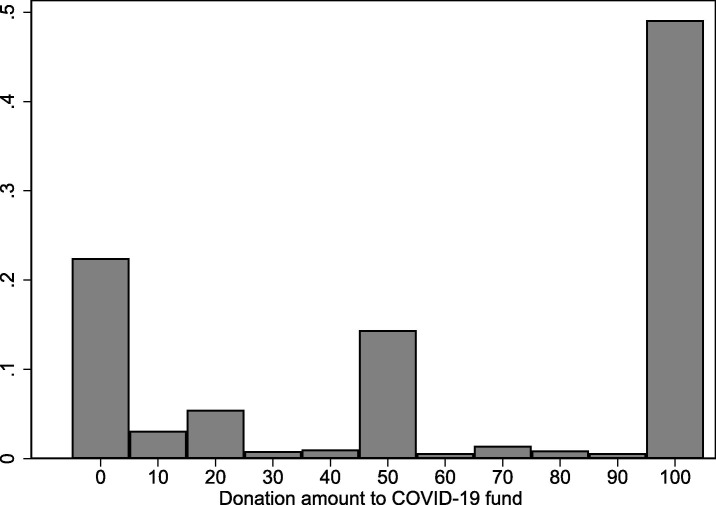
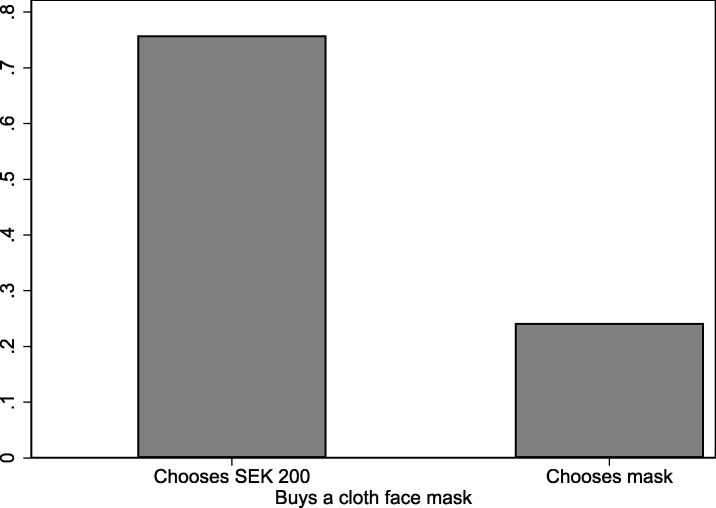
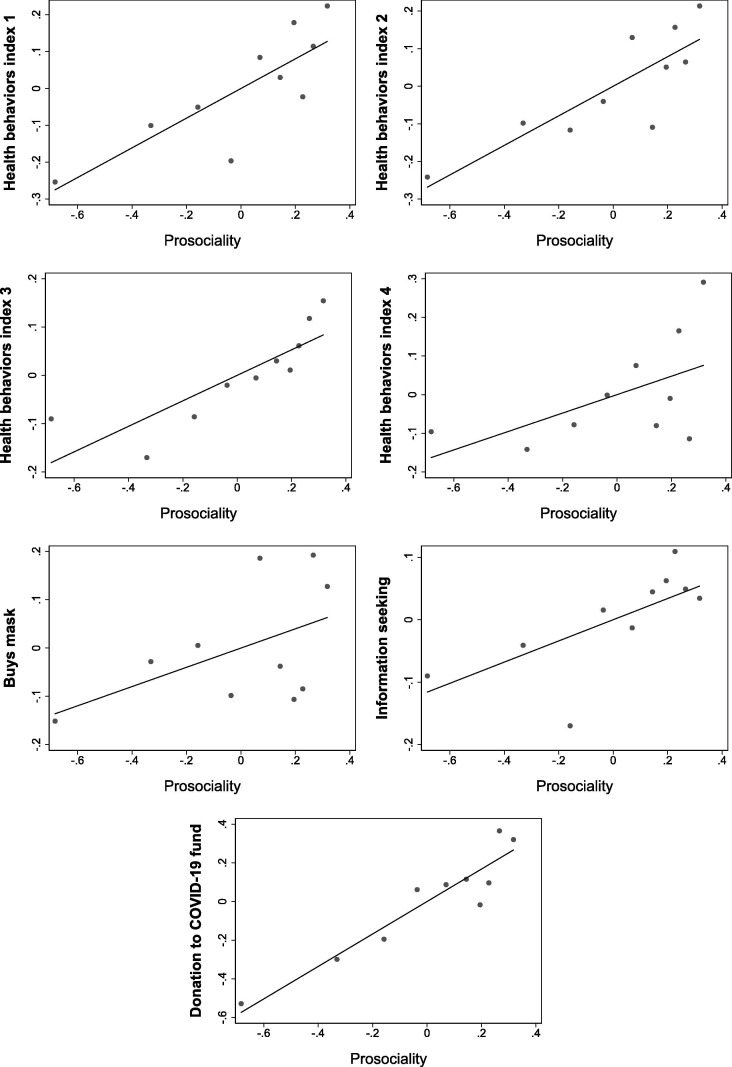
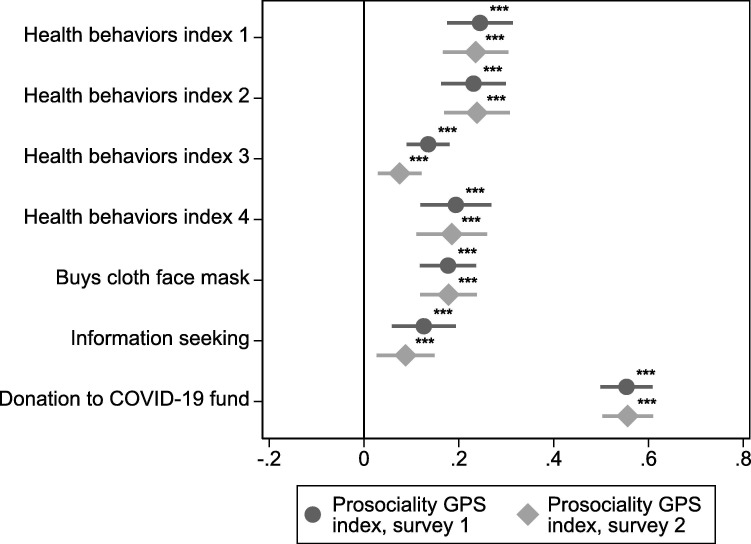
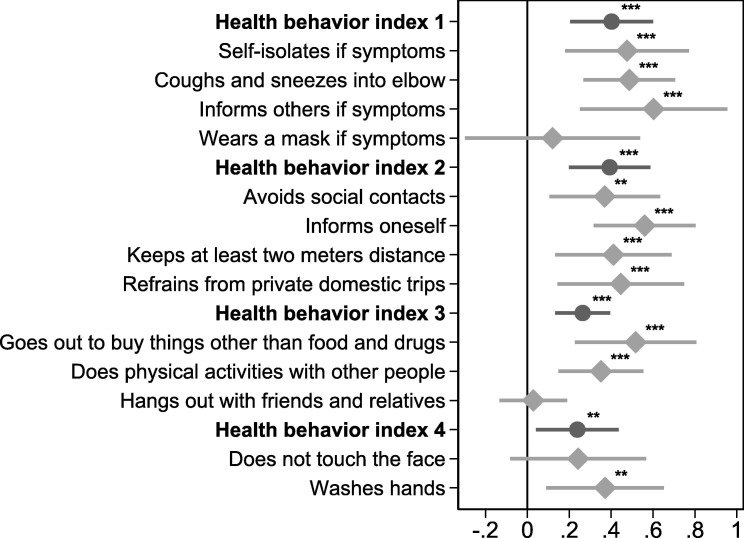
Socially responsible behavior is crucial for slowing the spread of infectious diseases. However, economic and epidemiological models of disease transmission abstract from prosocial motivations as a driver of behaviors that impact the health of others. In an incentivized study, we show that a large majority of people are very reluctant to put others at risk for their personal benefit. Moreover, this experimental measure of prosociality predicts health behaviors during the COVID-19 pandemic, measured in a separate and ostensibly unrelated study with the same people. Prosocial individuals are more likely to follow physical distancing guidelines, stay home when sick, and buy face masks. We also find that prosociality measured two years before the pandemic predicts health behaviors during the pandemic. Our findings indicate that prosociality is a stable, long-term predictor of policy-relevant behaviors, suggesting that the impact of policies on a population may depend on the degree of prosociality.
Keywords: COVID-19; Externalities; Health behavior; Prosociality; Social preferences.
© 2021 The Author(s).
Figures

Similar articles
-
Prosociality predicts individual behavior and collective outcomes in the COVID-19 pandemic.Soc Sci Med. 2022 Sep;308:115192. doi: 10.1016/j.socscimed.2022.115192. Epub 2022 Jul 8. Soc Sci Med. 2022. PMID: 35870298 Free PMC article.
-
Prosociality and health: Identification with all humanity is a replicable predictor of prosocial motivation for health behaviors.Front Psychol. 2023 Jan 12;13:1052713. doi: 10.3389/fpsyg.2022.1052713. eCollection 2022. Front Psychol. 2023. PMID: 36710834 Free PMC article.
-
Aging, Empathy, and Prosocial Behaviors During the COVID-19 Pandemic.J Gerontol B Psychol Sci Soc Sci. 2022 Apr 1;77(4):e57-e63. doi: 10.1093/geronb/gbab140. J Gerontol B Psychol Sci Soc Sci. 2022. PMID: 34320179 Free PMC article.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses.Cochrane Database Syst Rev. 2023 Jan 30;1(1):CD006207. doi: 10.1002/14651858.CD006207.pub6. Cochrane Database Syst Rev. 2023. PMID: 36715243 Free PMC article. Review.
-
Beyond good and evil: what motivations underlie children's prosocial behavior?Perspect Psychol Sci. 2015 Mar;10(2):159-75. doi: 10.1177/1745691615568998. Perspect Psychol Sci. 2015. PMID: 25910387 Review.
Cited by
-
Daily prosocial actions during the COVID-19 pandemic contribute to giving behavior in adolescence.Sci Rep. 2022 May 6;12(1):7458. doi: 10.1038/s41598-022-11421-3. Sci Rep. 2022. PMID: 35523982 Free PMC article.
-
Problem drinkers and high risk-taking behaviors under the stay-at-home policy of the COVID-19 emergency declaration.BMC Public Health. 2022 Jun 13;22(1):1173. doi: 10.1186/s12889-022-13331-5. BMC Public Health. 2022. PMID: 35692058 Free PMC article.
-
Communicating with ethnic minorities during COVID-19: An experimental test of the effect of self-, ingroup-, and intergroup-focused messages.Heliyon. 2023 Jun;9(6):e16629. doi: 10.1016/j.heliyon.2023.e16629. Epub 2023 May 29. Heliyon. 2023. PMID: 37287611 Free PMC article.
-
Older adults across the globe exhibit increased prosocial behavior but also greater in-group preferences.Nat Aging. 2021 Oct;1(10):880-888. doi: 10.1038/s43587-021-00118-3. Epub 2021 Oct 11. Nat Aging. 2021. PMID: 37118329 Free PMC article.
-
Willingness to give amid pandemics: a contingent valuation of anticipated nongovernmental immunization programs.Int J Health Econ Manag. 2022 Mar;22(1):53-68. doi: 10.1007/s10754-021-09309-2. Epub 2021 Jun 11. Int J Health Econ Manag. 2022. PMID: 34115255 Free PMC article.
References
-
- Alfaro, Laura, Faia, Ester, Lamersdorf, Nora, Saidi, Farzad, 2020. Social interactions in pandemics: Fear, altruism, and reciprocity. NBER WP No. 27134.
-
- Almås Ingvild, Cappelen Alexander W., Tungodden Bertil. Cutthroat capitalism versus cuddly Socialism: Are Americans more meritocratic and efficiency-seeking than Scandinavians? J. Polit. Econ. 2020;128(5):1753–1788.
-
- Anderson Lisa R., Mellor Jennifer M. Predicting health behaviors with an experimental measure of risk preference. J. Health Econ. 2008;27(5):1260–1274. - PubMed
-
- Andersson Ola, Holm Håkan J., Tyran Jean-Robert, Wengström Erik. Risking other people’s money: Experimental evidence on the role of incentives and personality traits. Scandinavian J. Econ. 2020;122(2):648–674.
-
- Andreoni James, Miller John. Giving According to GARP: An Experimental Test of the Consistency of Preferences for Altruism. Econometrica. 2002;70(2):737–753.
LinkOut - more resources
Full Text Sources
Other Literature Sources