

Potential Impact of Local Anesthetics Inducing Granulocyte Arrest and Altering Immune Functions on Perioperative Outcome
- PMID: 33442284
- PMCID: PMC7797324
- DOI: 10.2147/JIR.S275525
Potential Impact of Local Anesthetics Inducing Granulocyte Arrest and Altering Immune Functions on Perioperative Outcome
Abstract
Introduction: Local anesthetics (LAs) are frequently used during anesthesia; however, they may influence granulocyte function which in turn could modify immune responses in the perioperative period. Therefore, the aim of this study was to investigate the impact of clinically used doses of bupivacaine and lidocaine on granulocyte function with regard to migration, reactive oxygen species (ROS) production, neutrophil extracellular traps (NETosis) formation, and viability.
Methods: A total of 38 granulocyte-enriched samples from healthy subjects were obtained by whole blood lysis. Polymorphonuclear neutrophil (PMN) samples were incubated simultaneously with different concentrations of either bupivacaine (0.03-3.16 mmol/L) or lidocaine (0.007-14.21 mmol/L), or without drug (control). Live cell imaging was conducted in order to observe granulocyte chemotaxis, migration, ROS production, and NETosis. Flow cytometry was used to analyze viability and antigen expression.
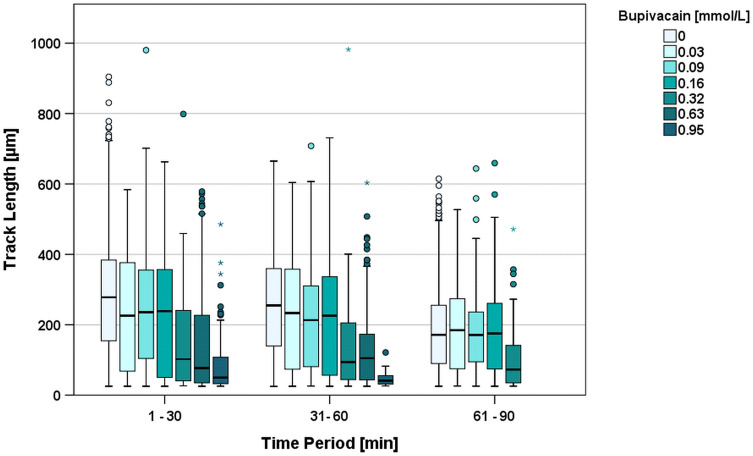
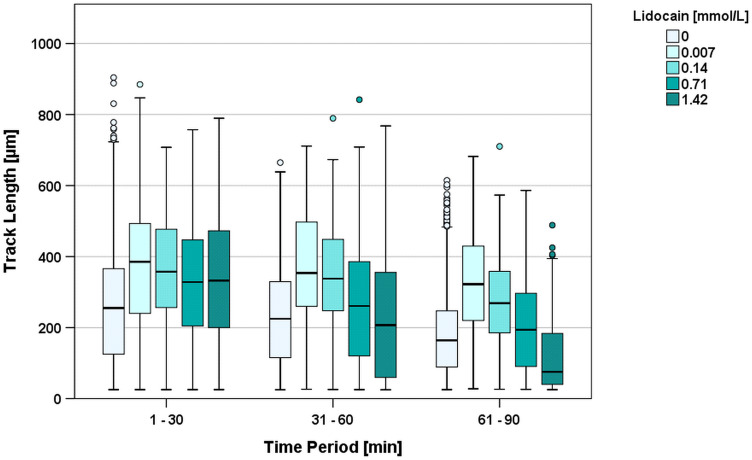
Results: The track length (TL) of PMNs exposed to bupivacaine concentrations of 0.16 mmol/L and above significantly decreased compared to the control. Low concentrations of lidocaine were associated with slight but significant increases in TL, whereas this changed with concentrations above 1.4 mmol/L, showing a significant decrease in TL. PMN incubated with bupivacaine concentrations of 1.58 mmol/L and above or lidocaine concentrations of at least 3.6 mmol/L showed no migration or chemotaxis at all. Time to onset of maximal ROS production and time for half-maximal NETosis decreased in a dose-dependent manner for both substances. Equipotency in NETosis induction was reached by bupivacaine (1.1 mmol/L) at significantly lower concentrations than lidocaine (7.96 mmol/L). Cell viability and oxidative burst were unaffected by LAs.
Conclusion: Local anesthetics in clinically used doses ameliorate granulocyte defense mechanisms, thus indicating their potentially decisive effect during the perioperative period.
Keywords: granulocytes; immune modulation; inflammation; local anesthetics; surgical trauma.
© 2021 Kolle et al.
Conflict of interest statement
The authors declare no conflicts of interest. Parts of this work were presented as an abstract at the Deutscher Anaesthesiecongress 2019 (German Anesthesiology Congress 2019) in Leipzig, Germany.
Figures


Similar articles
-
The Effect of Local Anesthetics on Neutrophils in the Context of Different Isolation Techniques.Biomedicines. 2023 Aug 2;11(8):2170. doi: 10.3390/biomedicines11082170. Biomedicines. 2023. PMID: 37626667 Free PMC article.
-
Propofol Ameliorates Exaggerated Human Neutrophil Activation in a LPS Sepsis Model.J Inflamm Res. 2021 Aug 11;14:3849-3862. doi: 10.2147/JIR.S314192. eCollection 2021. J Inflamm Res. 2021. PMID: 34408467 Free PMC article.
-
Effects of local anesthetics on the respiratory burst of cord blood neutrophils in vitro.Pediatr Res. 2016 Aug;80(2):258-66. doi: 10.1038/pr.2016.68. Epub 2016 Apr 7. Pediatr Res. 2016. PMID: 27055189
-
Impact of Nitric Oxide on Polymorphonuclear Neutrophils' Function.Biomedicines. 2024 Oct 16;12(10):2353. doi: 10.3390/biomedicines12102353. Biomedicines. 2024. PMID: 39457665 Free PMC article.
-
[Peribulbar anesthesia versus retrobulbar anesthesia with facial nerve block. Techniques, local anesthetics and additives, akinesia and sensory block, complications].Klin Monbl Augenheilkd. 1994 Feb;204(2):75-89. doi: 10.1055/s-2008-1035503. Klin Monbl Augenheilkd. 1994. PMID: 8170098 Review. German.
Cited by
-
The impact of stress and anesthesia on animal models of infectious disease.Front Vet Sci. 2023 Feb 2;10:1086003. doi: 10.3389/fvets.2023.1086003. eCollection 2023. Front Vet Sci. 2023. PMID: 36816193 Free PMC article. Review.
-
The effect of local anaesthetics on apoptosis and NETosis of human neutrophils in vitro: comparison between lidocaine and ropivacaine.Hum Cell. 2023 Nov;36(6):2027-2039. doi: 10.1007/s13577-023-00963-x. Epub 2023 Aug 17. Hum Cell. 2023. PMID: 37589878 Free PMC article.
-
The Effect of Local Anesthetics on Neutrophils in the Context of Different Isolation Techniques.Biomedicines. 2023 Aug 2;11(8):2170. doi: 10.3390/biomedicines11082170. Biomedicines. 2023. PMID: 37626667 Free PMC article.
-
Circulating biomarkers in perioperative management of cancer patients.Precis Clin Med. 2023 Jun 30;6(3):pbad018. doi: 10.1093/pcmedi/pbad018. eCollection 2023 Sep. Precis Clin Med. 2023. PMID: 37954451 Free PMC article. Review.
-
Propofol Ameliorates Exaggerated Human Neutrophil Activation in a LPS Sepsis Model.J Inflamm Res. 2021 Aug 11;14:3849-3862. doi: 10.2147/JIR.S314192. eCollection 2021. J Inflamm Res. 2021. PMID: 34408467 Free PMC article.
References
-
- Ates İ, Aydin ME, Ahiskalioglu A, Ahiskalioglu EO, Kaya Z, Gozeler MS. Postoperative analgesic efficacy of perioperative intravenous lidocaine infusion in patients undergoing septorhinoplasty: a prospective, randomized, double-blind study. Eur Arch Otorhinolaryngol. 2020;277(4):1095–1100. doi:10.1007/s00405-020-05801-6. - DOI - PubMed
-
- Poffers M, Bühne N, Herzog C, et al. Sodium channel Nav1.3 is expressed by polymorphonuclear neutrophils during mouse heart and kidney ischemia in vivo and regulates adhesion, transmigration, and chemotaxis of human and mouse neutrophils in vitro. Anesthesiology. 2018;128(6):1151–1166. doi:10.1097/ALN.0000000000002135. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
