

Determining if Telehealth Can Reduce Health System Costs: Scoping Review
- PMID: 33074157
- PMCID: PMC7605980
- DOI: 10.2196/17298
Determining if Telehealth Can Reduce Health System Costs: Scoping Review
Abstract
Background: Telehealth represents an opportunity for Australia to harness the power of technology to redesign the way health care is delivered. The potential benefits of telehealth include increased accessibility to care, productivity gains for health providers and patients through reduced travel, potential for cost savings, and an opportunity to develop culturally appropriate services that are more sensitive to the needs of special populations. The uptake of telehealth has been hindered at times by clinician reluctance and policies that preclude metropolitan populations from accessing telehealth services.
Objective: This study aims to investigate if telehealth reduces health system costs compared with traditional service models and to identify the scenarios in which cost savings can be realized.
Methods: A scoping review was undertaken to meet the study aims. Initially, literature searches were conducted using broad terms for telehealth and economics to identify economic evaluation literature in telehealth. The investigators then conducted an expert focus group to identify domains where telehealth could reduce health system costs, followed by targeted literature searches for corresponding evidence.
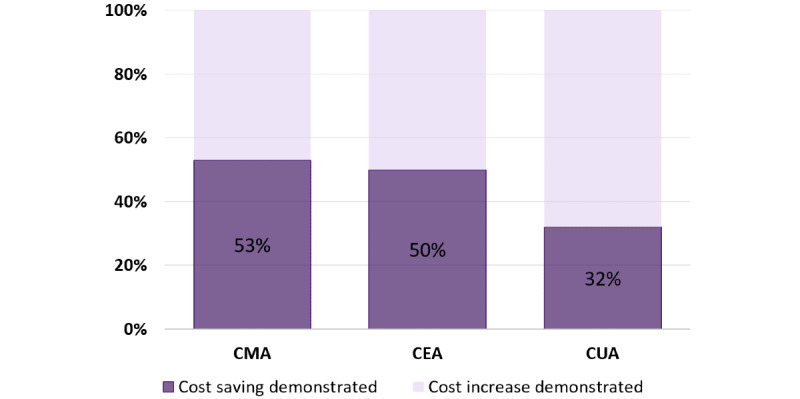
Results: The cost analyses reviewed provided evidence that telehealth reduced costs when health system-funded travel was prevented and when telehealth mitigated the need for expensive procedural or specialist follow-up by providing competent care in a more efficient way. The expert focus group identified 4 areas of potential savings from telehealth: productivity gains, reductions in secondary care, alternate funding models, and telementoring. Telehealth demonstrated great potential for productivity gains arising from health system redesign; however, under the Australian activity-based funding, it is unlikely that these gains will result in cost savings. Secondary care use mitigation is an area of promise for telehealth; however, many studies have not demonstrated overall cost savings due to the cost of administering and monitoring telehealth systems. Alternate funding models from telehealth systems have the potential to save the health system money in situations where the consumers pay out of pocket to receive services. Telementoring has had minimal economic evaluation; however, in the long term it is likely to result in inadvertent cost savings through the upskilling of generalist and allied health clinicians.
Conclusions: Health services considering implementing telehealth should be motivated by benefits other than cost reduction. The available evidence has indicated that although telehealth provides overwhelmingly positive patient benefits and increases productivity for many services, current evidence suggests that it does not routinely reduce the cost of care delivery for the health system.
Keywords: cost-benefit analysis; review; telemedicine.
©Centaine L Snoswell, Monica L Taylor, Tracy A Comans, Anthony C Smith, Leonard C Gray, Liam J Caffery. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 19.10.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

Similar articles
-
Exploring conceptual and theoretical frameworks for nurse practitioner education: a scoping review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):146-55. doi: 10.11124/jbisrir-2015-2150. JBI Database System Rev Implement Rep. 2015. PMID: 26571290
-
Defining the optimum strategy for identifying adults and children with coeliac disease: systematic review and economic modelling.Health Technol Assess. 2022 Oct;26(44):1-310. doi: 10.3310/ZUCE8371. Health Technol Assess. 2022. PMID: 36321689 Free PMC article.
-
Abrocitinib, tralokinumab and upadacitinib for treating moderate-to-severe atopic dermatitis.Health Technol Assess. 2024 Jan;28(4):1-113. doi: 10.3310/LEXB9006. Health Technol Assess. 2024. PMID: 38343072 Free PMC article.
-
The effectiveness of school-based family asthma educational programs on the quality of life and number of asthma exacerbations of children aged five to 18 years diagnosed with asthma: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):69-81. doi: 10.11124/jbisrir-2015-2335. JBI Database System Rev Implement Rep. 2015. PMID: 26571284
-
Depressing time: Waiting, melancholia, and the psychoanalytic practice of care.In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. In: Kirtsoglou E, Simpson B, editors. The Time of Anthropology: Studies of Contemporary Chronopolitics. Abingdon: Routledge; 2020. Chapter 5. PMID: 36137063 Free Books & Documents. Review.
Cited by
-
Telehealth implementation for children with attention deficit hyperactivity disorder: a scoping review.Child Health Nurs Res. 2024 Oct;30(4):227-244. doi: 10.4094/chnr.2024.026. Epub 2024 Oct 31. Child Health Nurs Res. 2024. PMID: 39477230 Free PMC article.
-
The Calm after the Storm: A State-of-the-Art Review about Recommendations Put Forward during the COVID-19 Pandemic to Improve Chronic Pain Management.J Clin Med. 2023 Nov 22;12(23):7233. doi: 10.3390/jcm12237233. J Clin Med. 2023. PMID: 38068285 Free PMC article. Review.
-
COVID-19 pandemic effects on the distribution of healthcare services in India: A systematic review.World J Virol. 2022 Jul 25;11(4):186-197. doi: 10.5501/wjv.v11.i4.186. World J Virol. 2022. PMID: 36159611 Free PMC article.
-
Physiotherapist-led, exercise-based telerehabilitation for older adults improves patient and health service outcomes: a systematic review and meta-analysis.Age Ageing. 2023 Nov 2;52(11):afad207. doi: 10.1093/ageing/afad207. Age Ageing. 2023. PMID: 37979183 Free PMC article.
-
Greenway of Digital Health Technology During COVID-19 Crisis: Bibliometric Analysis, Challenges, and Future Perspective.Adv Exp Med Biol. 2024;1458:315-334. doi: 10.1007/978-3-031-61943-4_21. Adv Exp Med Biol. 2024. PMID: 39102206 Review.
References
-
- Australian Institute of Health and Welfare . AIHW. Canberra: Australian Government; 2018. Sep 28, [2018-12-31]. Health expenditure Australia 2016-17. https://www.aihw.gov.au/reports/health-welfare-expenditure/health-expend... www.aihw.gov.au/reports/health-welfare-expenditure/health-expenditure-au....
-
- Centers for Medicare and Medicaid Services National Health Expenditure Data. CMS. 2018. [2019-11-26]. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Tren....
-
- Bilinski A, Neumann P, Cohen J, Thorat T, McDaniel K, Salomon JA. When cost-effective interventions are unaffordable: integrating cost-effectiveness and budget impact in priority setting for global health programs. PLoS Med. 2017 Oct;14(10):e1002397. doi: 10.1371/journal.pmed.1002397. https://dx.plos.org/10.1371/journal.pmed.1002397 - DOI - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
