

Rapid humoral immune responses are required for recovery from haemorrhagic fever with renal syndrome patients
- PMID: 32990499
- PMCID: PMC8284976
- DOI: 10.1080/22221751.2020.1830717
Rapid humoral immune responses are required for recovery from haemorrhagic fever with renal syndrome patients
Abstract
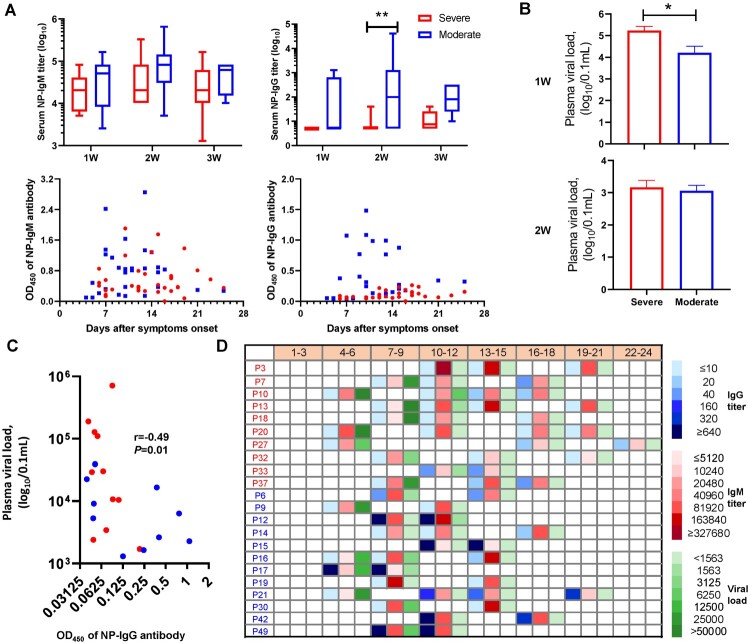
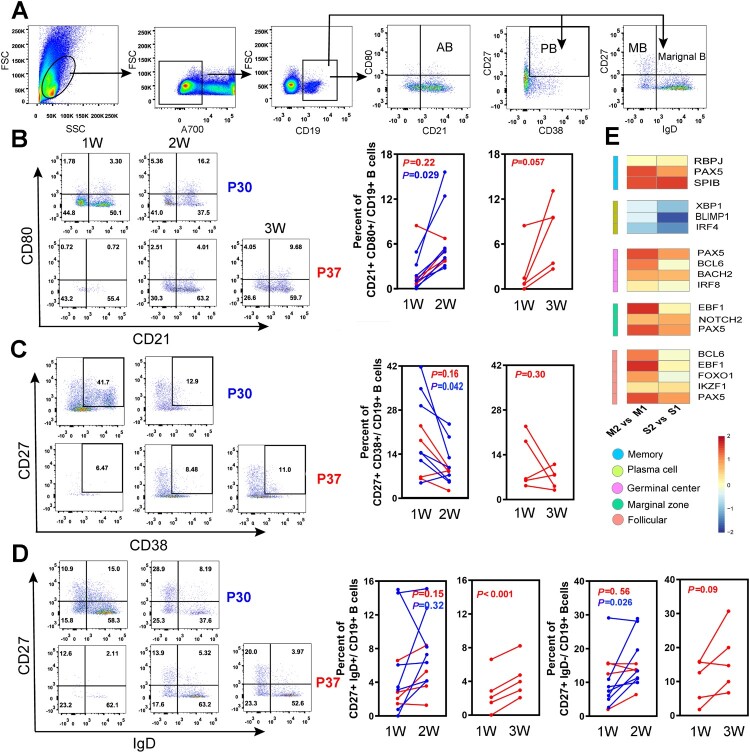
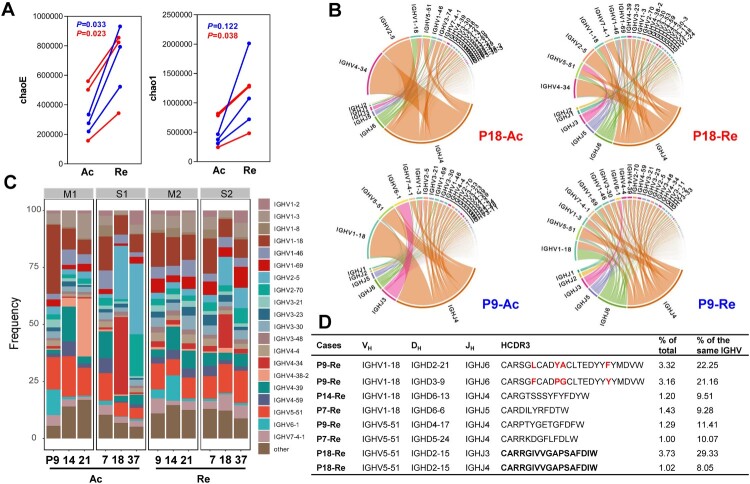
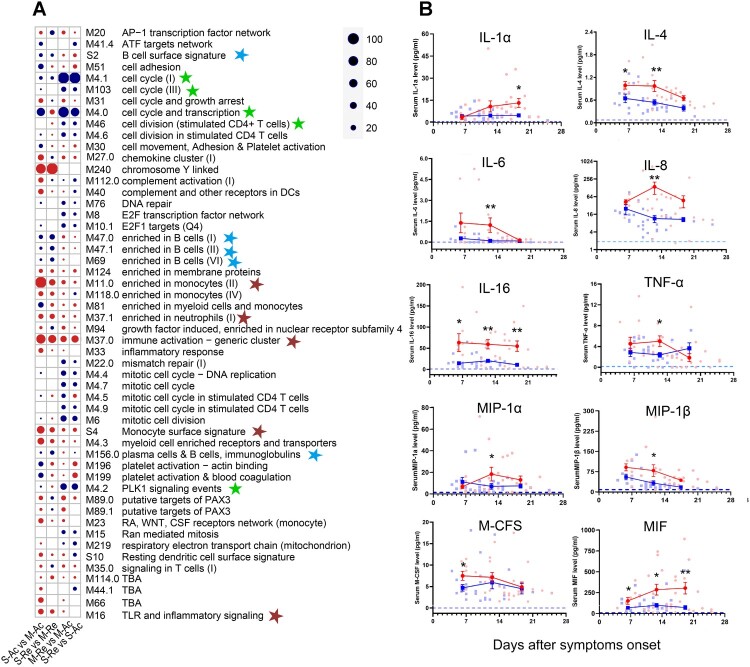
ABSTRACT Haemorrhagic fever with renal syndrome (HFRS) following Hantaan virus (HTNV) infection displays variable clinical signs. Humoral responses elicited during HTNV infections are considered important, however, this process remains poorly understood. Herein, we have investigated the phenotype, temporal dynamics, and characteristics of B-cell receptor (BCR) repertoire in an HFRS cohort. The serological profiles were characterized by a lowered expression level of nucleoprotein (NP)-specific antibody in severe cases. Importantly, B-cell subsets were activated and proliferated within the first two weeks of symptom onset and moderate cases reacted more rapidly. BCR analysis in the recovery phase revealed a dramatic increase in the immunoglobulin gene diversity which was more significantly progressed in moderate infections. In severe cases, B-cell-related transcription was lower with inflammatory sets overactivated. Taken together, these data suggest the clinical signs and disease recovery in HFRS patients were positively impacted by rapid and efficacious humoral responses.
Keywords: B cell; Haemorrhagic fever with renal syndrome; Hantaan virus; humoral response; virus infection.
Conflict of interest statement
No potential conflict of interest was reported by the author(s). The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of manuscript, and in the decision to publish results.
Figures
Similar articles
-
The assessment of Hantaan virus-specific antibody responses after the immunization program for hemorrhagic fever with renal syndrome in northwest China.Hum Vaccin Immunother. 2017 Apr 3;13(4):802-807. doi: 10.1080/21645515.2016.1253645. Epub 2016 Nov 8. Hum Vaccin Immunother. 2017. PMID: 27824286 Free PMC article.
-
CD8low CD100- T Cells Identify a Novel CD8 T Cell Subset Associated with Viral Control during Human Hantaan Virus Infection.J Virol. 2015 Dec;89(23):11834-44. doi: 10.1128/JVI.01610-15. Epub 2015 Sep 16. J Virol. 2015. PMID: 26378166 Free PMC article.
-
Analysis of immune responses against nucleocapsid protein of the Hantaan virus elicited by virus infection or DNA vaccination.J Microbiol. 2005 Dec;43(6):537-45. J Microbiol. 2005. PMID: 16410771
-
Hanta hemorrhagic fever with renal syndrome: a case report and review.J Microbiol Immunol Infect. 2005 Jun;38(3):221-3. J Microbiol Immunol Infect. 2005. PMID: 15986074 Review.
-
Hemorrhagic Fever with Renal Syndrome: Pathogenesis and Clinical Picture.Front Cell Infect Microbiol. 2016 Feb 3;6:1. doi: 10.3389/fcimb.2016.00001. eCollection 2016. Front Cell Infect Microbiol. 2016. PMID: 26870699 Free PMC article. Review.
Cited by
-
Transcriptomic analysis reveals key molecular signatures across recovery phases of hemorrhagic fever with renal syndrome.BMC Med Genomics. 2024 Sep 11;17(1):229. doi: 10.1186/s12920-024-02004-4. BMC Med Genomics. 2024. PMID: 39261833 Free PMC article.
-
The Role of Nucleoprotein in Immunity to Human Negative-Stranded RNA Viruses-Not Just Another Brick in the Viral Nucleocapsid.Viruses. 2022 Mar 3;14(3):521. doi: 10.3390/v14030521. Viruses. 2022. PMID: 35336928 Free PMC article. Review.
-
Discovering common pathogenic processes between COVID-19 and HFRS by integrating RNA-seq differential expression analysis with machine learning.Front Microbiol. 2023 May 5;14:1175844. doi: 10.3389/fmicb.2023.1175844. eCollection 2023. Front Microbiol. 2023. PMID: 37234545 Free PMC article.
-
The differences in cytokine signatures between severe fever with thrombocytopenia syndrome (SFTS) and hemorrhagic fever with renal syndrome (HFRS).J Virol. 2024 Jul 23;98(7):e0078624. doi: 10.1128/jvi.00786-24. Epub 2024 Jun 25. J Virol. 2024. PMID: 38916398 Free PMC article.
References
-
- Song G. Epidemiological progresses of hemorrhagic fever with renal syndrome in China. Chin Med J. 1999 May;112(5):472–477. - PubMed
-
- Koivula TT, Tuulasvaara A, Hetemaki I, et al. . Regulatory T cell response correlates with the severity of human hantavirus infection. J Infect. 2014 Apr;68(4):387–394. - PubMed
-
- Chandy S, Mathai D.. Globally emerging hantaviruses: An overview. Indian J Med Microbiol. 2017 Apr–Jun;35(2):165–175. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous