

Determinants of suboptimal CD4+ T cell recovery after antiretroviral therapy initiation in a prospective cohort of acute HIV-1 infection
- PMID: 32949118
- PMCID: PMC7507109
- DOI: 10.1002/jia2.25585
Determinants of suboptimal CD4+ T cell recovery after antiretroviral therapy initiation in a prospective cohort of acute HIV-1 infection
Abstract
Introduction: Up to 30% of individuals treated with antiretroviral therapy (ART) during chronic HIV fail to recover CD4 counts to >500 cells/mm3 despite plasma viral suppression. We investigated the frequency and associations of suboptimal CD4 recovery after ART started during acute HIV infection (AHI).
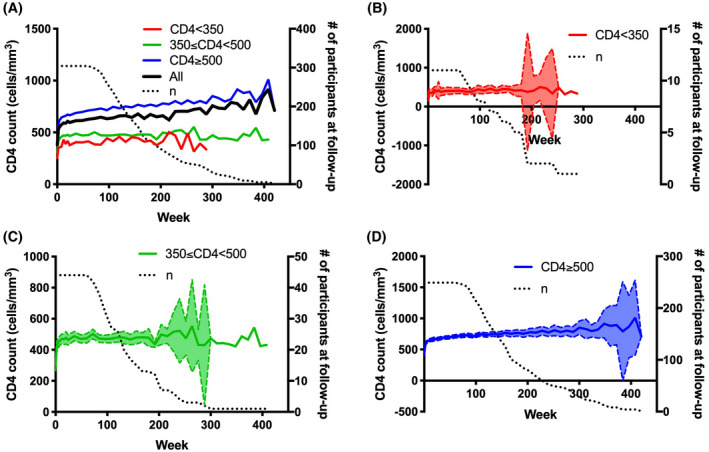
Methods: Participants who started ART in Fiebig I to V AHI with ≥48 weeks of continuous documented HIV-RNA < 50 copies/mL were stratified by CD4 count at latest study visit to suboptimal immune recovery (SIR; CD4 < 350 cells/mm3 ), intermediate immune recovery (IIR; 350 ≤ CD4 < 500) and complete immune recovery (CIR; CD4 ≥ 500). Clinical and laboratory parameters were assessed at pre-ART baseline and latest study visit. Additional inflammatory and neurobehavioral endpoints were examined at baseline and 96 weeks.
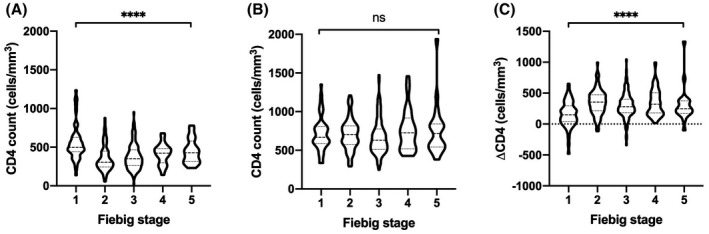
Results: Of 304 participants (96% male, median 26 years old) evaluated after median 144 (range 60 to 420) weeks of ART initiated at median 19 days (range 1 to 62) post-exposure, 3.6% (n = 11) had SIR and 14.5% (n = 44) had IIR. Pre-ART CD4 count in SIR compared to CIR participants was 265 versus 411 cells/mm3 (p = 0.002). Individuals with SIR or IIR had a slower CD4 rate of recovery compared to those with CIR. Timing of ART initiation by Fiebig stage did not affect CD4 count during treatment. Following ART, the CD8+ T cell count (p = 0.001) and CD4/CD8 ratio (p = 0.047) were lower in SIR compared to CIR participants. Compared to the CIR group at week 96, the combined SIR and IIR groups had higher sCD14 (p = 0.008) and lower IL-6 (p = 0.04) in plasma, without differences in neuropsychological or psychiatric indices.
Conclusions: Despite immediate and sustained treatment in AHI, suboptimal CD4 recovery occurs uncommonly and is associated with low pre-ART CD4 count as well as persistent low CD8 count and CD4/CD8 ratio during treatment.
Keywords: ARV; Asia; HIV care continuum; LMIC; immunology; men who have sex with men.
© 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of International AIDS Society.
Figures
Similar articles
-
Immune recovery in HIV-1 infected patients with sustained viral suppression under long-term antiretroviral therapy in Ethiopia.PLoS One. 2020 Oct 22;15(10):e0240880. doi: 10.1371/journal.pone.0240880. eCollection 2020. PLoS One. 2020. PMID: 33091053 Free PMC article.
-
Impact of CD8+ T-cell activation on CD4+ T-cell recovery and mortality in HIV-infected Ugandans initiating antiretroviral therapy.AIDS. 2011 Nov 13;25(17):2123-31. doi: 10.1097/QAD.0b013e32834c4ac1. AIDS. 2011. PMID: 21881481 Free PMC article.
-
Rapid CD4 decline prior to antiretroviral therapy predicts subsequent failure to reconstitute despite HIV viral suppression.J Infect Public Health. 2018 Mar-Apr;11(2):265-269. doi: 10.1016/j.jiph.2017.08.001. Epub 2017 Aug 18. J Infect Public Health. 2018. PMID: 28826735
-
Human immunodeficiency virus and the gastrointestinal immune system: does highly active antiretroviral therapy restore gut immunity?Mucosal Immunol. 2012 Nov;5(6):596-604. doi: 10.1038/mi.2012.82. Epub 2012 Aug 29. Mucosal Immunol. 2012. PMID: 22929559 Review.
-
Plasma concentrations of IL-6, MIP-1β, IP-10, and PTX-3 as predictors of the immunological response to antiretroviral treatment in people with HIV.Front Immunol. 2024 Aug 29;15:1447926. doi: 10.3389/fimmu.2024.1447926. eCollection 2024. Front Immunol. 2024. PMID: 39267754 Free PMC article. Review.
Cited by
-
Safety and Immunogenicity of Inactivated COVID-19 Vaccines Among People Living with HIV in China.Infect Drug Resist. 2022 Apr 21;15:2091-2100. doi: 10.2147/IDR.S353127. eCollection 2022. Infect Drug Resist. 2022. PMID: 35480056 Free PMC article.
-
Factors Associated with Neutralizing Antibody Responses following 2-Dose and 3rd Booster Monovalent COVID-19 Vaccination in Japanese People Living with HIV.Viruses. 2024 Apr 2;16(4):555. doi: 10.3390/v16040555. Viruses. 2024. PMID: 38675897 Free PMC article.
-
Evaluation of antiretroviral therapy effect and prognosis between HIV-1 recent and long-term infection based on a rapid recent infection testing algorithm.Front Microbiol. 2022 Nov 22;13:1004960. doi: 10.3389/fmicb.2022.1004960. eCollection 2022. Front Microbiol. 2022. PMID: 36483196 Free PMC article.
-
Recent advances in poor HIV immune reconstitution: what will the future look like?Front Microbiol. 2023 Aug 7;14:1236460. doi: 10.3389/fmicb.2023.1236460. eCollection 2023. Front Microbiol. 2023. PMID: 37608956 Free PMC article. Review.
-
Evaluation of Clinical Biomarkers Related to CD4 Recovery in HIV-Infected Patients-5-Year Observation.Viruses. 2022 Oct 18;14(10):2287. doi: 10.3390/v14102287. Viruses. 2022. PMID: 36298842 Free PMC article.
References
-
- Gazzola L, Tincati C, Bellistri GM, Monforte A, Marchetti G. The absence of CD4+ T cell count recovery despite receipt of virologically suppressive highly active antiretroviral therapy: clinical risk, immunological gaps, and therapeutic options. Clin Infect Dis. 2009;48(3):328–37. - PubMed
-
- Hocqueloux L, Avettand‐Fenoel V, Jacquot S, Prazuck T, Legac E, Melard A, et al. Long‐term antiretroviral therapy initiated during primary HIV‐1 infection is key to achieving both low HIV reservoirs and normal T cell counts. J Antimicrob Chemother. 2013;68(5):1169–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
