

Shedding of SARS-CoV-2 in feces and urine and its potential role in person-to-person transmission and the environment-based spread of COVID-19
- PMID: 32836117
- PMCID: PMC7836549
- DOI: 10.1016/j.scitotenv.2020.141364
Shedding of SARS-CoV-2 in feces and urine and its potential role in person-to-person transmission and the environment-based spread of COVID-19
Abstract
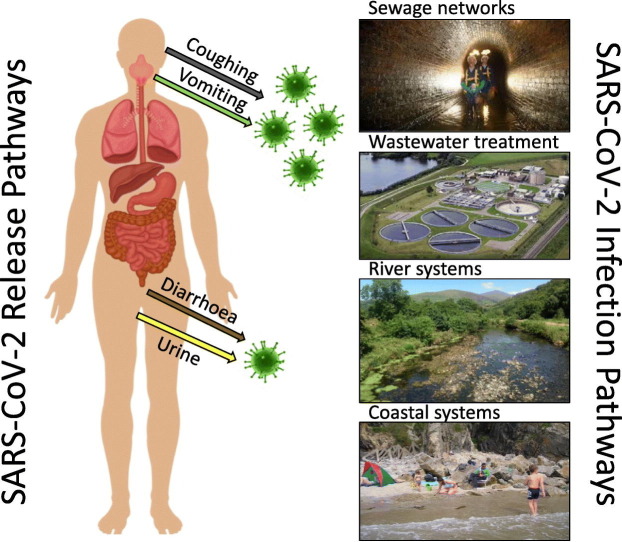
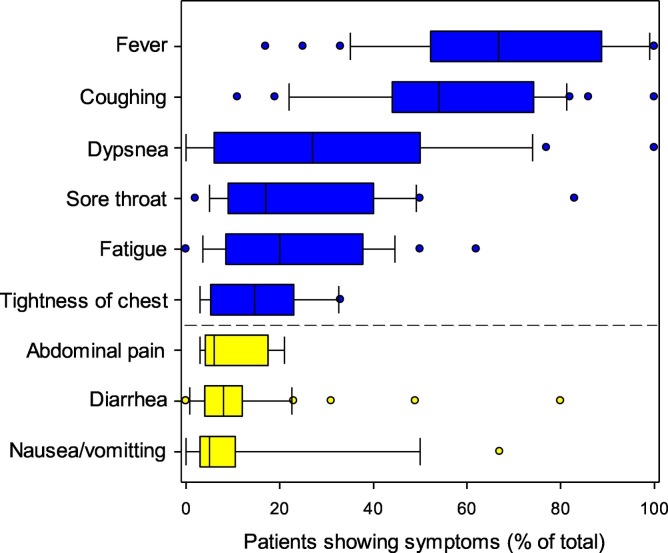
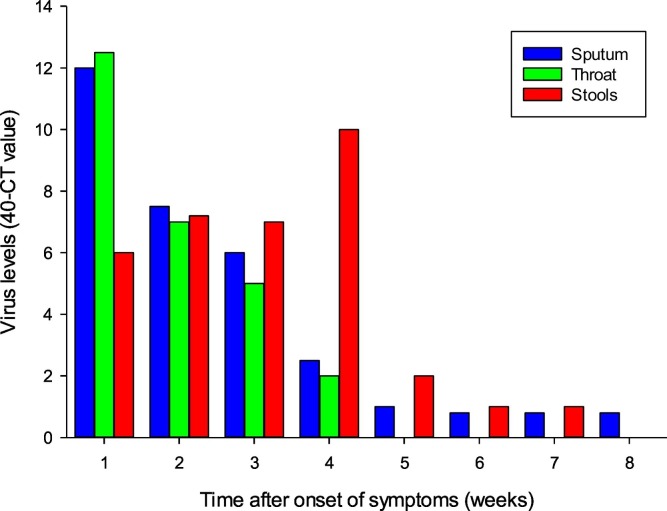
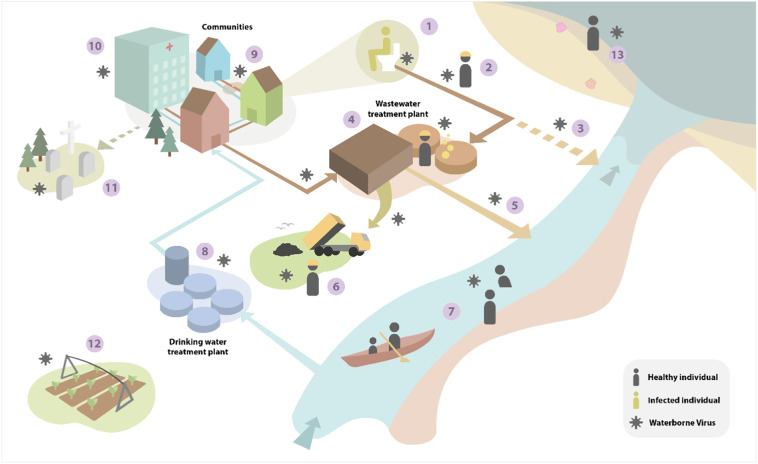
The recent detection of SARS-CoV-2 RNA in feces has led to speculation that it can be transmitted via the fecal-oral/ocular route. This review aims to critically evaluate the incidence of gastrointestinal (GI) symptoms, the quantity and infectivity of SARS-CoV-2 in feces and urine, and whether these pose an infection risk in sanitary settings, sewage networks, wastewater treatment plants, and the wider environment (e.g. rivers, lakes and marine waters). A review of 48 independent studies revealed that severe GI dysfunction is only evident in a small number of COVID-19 cases, with 11 ± 2% exhibiting diarrhea and 12 ± 3% exhibiting vomiting and nausea. In addition to these cases, SARS-CoV-2 RNA can be detected in feces from some asymptomatic, mildly- and pre-symptomatic individuals. Fecal shedding of the virus peaks in the symptomatic period and can persist for several weeks, but with declining abundances in the post-symptomatic phase. SARS-CoV-2 RNA is occasionally detected in urine, but reports in fecal samples are more frequent. The abundance of the virus genetic material in both urine (ca. 102-105 gc/ml) and feces (ca. 102-107 gc/ml) is much lower than in nasopharyngeal fluids (ca. 105-1011 gc/ml). There is strong evidence of multiplication of SARS-CoV-2 in the gut and infectious virus has occasionally been recovered from both urine and stool samples. The level and infectious capability of SARS-CoV-2 in vomit remain unknown. In comparison to enteric viruses transmitted via the fecal-oral route (e.g. norovirus, adenovirus), the likelihood of SARS-CoV-2 being transmitted via feces or urine appears much lower due to the lower relative amounts of virus present in feces/urine. The biggest risk of transmission will occur in clinical and care home settings where secondary handling of people and urine/fecal matter occurs. In addition, while SARS-CoV-2 RNA genetic material can be detected by in wastewater, this signal is greatly reduced by conventional treatment. Our analysis also suggests the likelihood of infection due to contact with sewage-contaminated water (e.g. swimming, surfing, angling) or food (e.g. salads, shellfish) is extremely low or negligible based on very low predicted abundances and limited environmental survival of SARS-CoV-2. These conclusions are corroborated by the fact that tens of million cases of COVID-19 have occurred globally, but exposure to feces or wastewater has never been implicated as a transmission vector.
Keywords: Bathing waters; Fecal-oral route; Infection risk; Sanitation; Waterborne illness.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


Similar articles
-
Detection of SARS-CoV-2 in Fecal Samples From Patients With Asymptomatic and Mild COVID-19 in Korea.Clin Gastroenterol Hepatol. 2021 Jul;19(7):1387-1394.e2. doi: 10.1016/j.cgh.2020.06.005. Epub 2020 Jun 10. Clin Gastroenterol Hepatol. 2021. PMID: 32534042 Free PMC article.
-
Enumerating asymptomatic COVID-19 cases and estimating SARS-CoV-2 fecal shedding rates via wastewater-based epidemiology.Sci Total Environ. 2021 Dec 20;801:149794. doi: 10.1016/j.scitotenv.2021.149794. Epub 2021 Aug 20. Sci Total Environ. 2021. PMID: 34467933 Free PMC article.
-
Prevalence of Gastrointestinal Symptoms and Fecal Viral Shedding in Patients With Coronavirus Disease 2019: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Jun 1;3(6):e2011335. doi: 10.1001/jamanetworkopen.2020.11335. JAMA Netw Open. 2020. PMID: 32525549 Free PMC article.
-
Intestinal viral infections of nSARS-CoV2 in the Indian community: Risk of virus spread in India.J Med Virol. 2022 Apr;94(4):1315-1329. doi: 10.1002/jmv.27480. Epub 2021 Dec 3. J Med Virol. 2022. PMID: 34825708 Free PMC article. Review.
-
Absence of virological and epidemiological evidence that SARS-CoV-2 poses COVID-19 risks from environmental fecal waste, wastewater and water exposures.J Water Health. 2022 Jan;20(1):126-138. doi: 10.2166/wh.2021.182. J Water Health. 2022. PMID: 35100160 Review.
Cited by
-
Longitudinal wastewater-based surveillance of SARS-CoV-2 during 2023 in Ethiopia.Front Public Health. 2024 Oct 7;12:1394798. doi: 10.3389/fpubh.2024.1394798. eCollection 2024. Front Public Health. 2024. PMID: 39435409 Free PMC article.
-
Longitudinal fecal shedding of SARS-CoV-2, pepper mild mottle virus, and human mitochondrial DNA in COVID-19 patients.Front Med (Lausanne). 2024 Sep 11;11:1417967. doi: 10.3389/fmed.2024.1417967. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39323476 Free PMC article.
-
The first detection of SARS-CoV-2 RNA in the wastewater of Bucharest, Romania.Sci Rep. 2024 Sep 17;14(1):21730. doi: 10.1038/s41598-024-72854-6. Sci Rep. 2024. PMID: 39289536 Free PMC article.
-
Fecal shedding of SARS-CoV-2 in infants born to SARS-CoV-2 positive mothers: a pilot study.PeerJ. 2024 Aug 27;12:e17956. doi: 10.7717/peerj.17956. eCollection 2024. PeerJ. 2024. PMID: 39221275 Free PMC article.
-
Use of wastewater from passenger ships to assess the movement of COVID-19 and other pathogenic viruses across maritime international boundaries.Front Public Health. 2024 Jul 15;12:1377996. doi: 10.3389/fpubh.2024.1377996. eCollection 2024. Front Public Health. 2024. PMID: 39076415 Free PMC article.
References
-
- Adhikari S.P., Meng S., Wu Y., Mao Y., Ye R., Wang Q., Sun C., Sylvia S., Rozelle S., Raat H., Zhou H. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect. Dis. Poverty. 2020;9:29. doi: 10.1186/s40249-020-00646-x. - DOI - PMC - PubMed
-
- Ahmed W., Angel N., Edson J., Bibby K., Bivins A., O’Brien J.W., Choi P.M., Kitajima M., Simpson S.L., Li J., Tscharke B., Verhagen R., Smith W.J.M., Zaugg J., Dierens L., Hugenholtz P., Thomas K.V., Mueller J.F. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: a proof of concept for the wastewater surveillance of COVID-19 in the community. Sci. Total Environ. 2020;728 doi: 10.1016/j.scitotenv.2020.138764. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
