

Therapy of Parkinson's Disease Subtypes
- PMID: 32749651
- PMCID: PMC7851253
- DOI: 10.1007/s13311-020-00894-7
Therapy of Parkinson's Disease Subtypes
Abstract
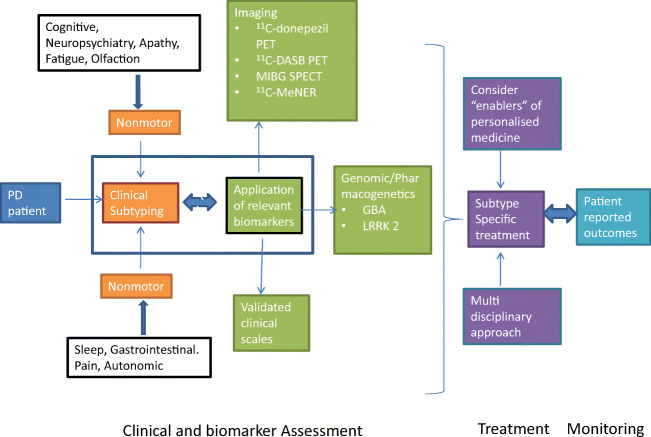
Early descriptions of subtypes of Parkinson's disease (PD) are dominated by the approach of predetermined groups. Experts defined, from clinical observation, groups based on clinical or demographic features that appeared to divide PD into clinically distinct subsets. Common bases on which to define subtypes have been motor phenotype (tremor dominant vs akinetic-rigid or postural instability gait disorder types), age, nonmotor dominant symptoms, and genetic forms. Recently, data-driven approaches have been used to define PD subtypes, taking an unbiased statistical approach to the identification of PD subgroups. The vast majority of data-driven subtyping has been done based on clinical features. Biomarker-based subtyping is an emerging but still quite undeveloped field. Not all of the subtyping methods have established therapeutic implications. This may not be surprising given that they were born largely from clinical observations of phenotype and not in observations regarding treatment response or biological hypotheses. The next frontier for subtypes research as it applies to personalized medicine in PD is the development of genotype-specific therapies. Therapies for GBA-PD and LRRK2-PD are already under development. This review discusses each of the major subtyping systems/methods in terms of its applicability to therapy in PD, and the opportunities and challenges designing clinical trials to develop the evidence base for personalized medicine based on subtypes.
Keywords: Parkinson’s disease; subtypes; therapy.
Figures
Similar articles
-
Nonmotor features of Parkinson's disease subtypes.Mov Disord. 2016 Aug;31(8):1095-102. doi: 10.1002/mds.26510. Epub 2016 Feb 10. Mov Disord. 2016. PMID: 26861861 Review.
-
Clinical and Dopamine Transporter Imaging Characteristics of Leucine Rich Repeat Kinase 2 (LRRK2) and Glucosylceramidase Beta (GBA) Parkinson's Disease Participants in the Parkinson's Progression Markers Initiative: A Cross-Sectional Study.Mov Disord. 2020 May;35(5):833-844. doi: 10.1002/mds.27989. Epub 2020 Feb 19. Mov Disord. 2020. PMID: 32073681 Free PMC article.
-
Precision medicine in Parkinson's disease patients with LRRK2 and GBA risk variants - Let's get even more personal.Transl Neurodegener. 2020 Oct 16;9(1):39. doi: 10.1186/s40035-020-00218-x. Transl Neurodegener. 2020. PMID: 33066808 Free PMC article. Review.
-
New therapeutic approaches to Parkinson's disease targeting GBA, LRRK2 and Parkin.Neuropharmacology. 2022 Jan 1;202:108822. doi: 10.1016/j.neuropharm.2021.108822. Epub 2021 Oct 7. Neuropharmacology. 2022. PMID: 34626666 Review.
-
Approaches to Early Parkinson's Disease Subtyping.J Parkinsons Dis. 2024;14(s2):S297-S306. doi: 10.3233/JPD-230419. J Parkinsons Dis. 2024. PMID: 39331104 Free PMC article. Review.
Cited by
-
Tremor in Parkinson's Disease: From Pathophysiology to Advanced Therapies.Tremor Other Hyperkinet Mov (N Y). 2022 Sep 13;12:29. doi: 10.5334/tohm.712. eCollection 2022. Tremor Other Hyperkinet Mov (N Y). 2022. PMID: 36211804 Free PMC article. Review.
-
Nonmotor symptom burden grading as predictor of cognitive impairment in Parkinson's disease.Brain Behav. 2021 May;11(5):e02086. doi: 10.1002/brb3.2086. Epub 2021 Mar 1. Brain Behav. 2021. PMID: 33645912 Free PMC article.
-
Individual Magnetoencephalography Response Profiles to Short-Duration L-Dopa in Parkinson's Disease.Front Hum Neurosci. 2021 Mar 15;15:640591. doi: 10.3389/fnhum.2021.640591. eCollection 2021. Front Hum Neurosci. 2021. PMID: 33790752 Free PMC article.
-
Does Depression Contribute to the Bladder and Bowel Complaint in Parkinson's Disease Patients?Mov Disord Clin Pract. 2020 Dec 27;8(2):240-244. doi: 10.1002/mdc3.13124. eCollection 2021 Feb. Mov Disord Clin Pract. 2020. PMID: 33553494 Free PMC article.
-
Intraperitoneal Administration of Forskolin Reverses Motor Symptoms and Loss of Midbrain Dopamine Neurons in PINK1 Knockout Rats.J Parkinsons Dis. 2022;12(3):831-850. doi: 10.3233/JPD-213016. J Parkinsons Dis. 2022. PMID: 34957950 Free PMC article.
References
-
- Parkinson J. An essay on the shaking palsy. 1817. The Journal of neuropsychiatry and clinical neurosciences. 2002;14(2):223–36. - PubMed
-
- Fahn S. The history of parkinsonism. Movement Disorders. 1989;4(S1):S2–S10. - PubMed
-
- Weiner WJ. There is no Parkinson disease. Archives of neurology. 2008;65(6):705–8. - PubMed
-
- Jankovic J, McDermott M, Carter J, Gauthier S, Goetz C, Golbe L, et al. Variable expression of Parkinson’s disease: a base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology. 1990;40(10):1529–34. - PubMed
-
- Zetusky WJ, Jankovic J, Pirozzolo FJ. The heterogeneity of Parkinson’s disease: clinical and prognostic implications. Neurology. 1985;35(4):522–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
