

Targeting GM-CSF in COVID-19 Pneumonia: Rationale and Strategies
- PMID: 32719685
- PMCID: PMC7348297
- DOI: 10.3389/fimmu.2020.01625
Targeting GM-CSF in COVID-19 Pneumonia: Rationale and Strategies
Abstract
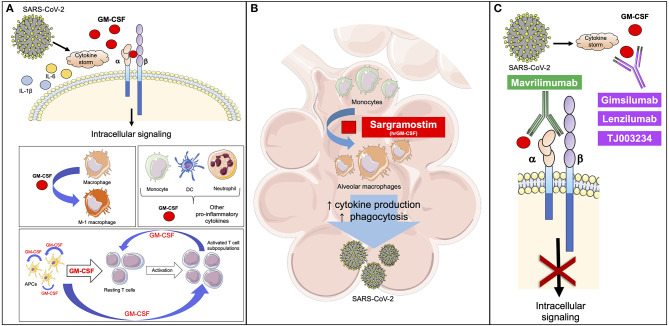
COVID-19 is a clinical syndrome ranging from mild symptoms to severe pneumonia that often leads to respiratory failure, need for mechanical ventilation, and death. Most of the lung damage is driven by a surge in inflammatory cytokines [interleukin-6, interferon-γ, and granulocyte-monocyte stimulating factor (GM-CSF)]. Blunting this hyperinflammation with immunomodulation may lead to clinical improvement. GM-CSF is produced by many cells, including macrophages and T-cells. GM-CSF-derived signals are involved in differentiation of macrophages, including alveolar macrophages (AMs). In animal models of respiratory infections, the intranasal administration of GM-CSF increased the proliferation of AMs and improved outcomes. Increased levels of GM-CSF have been recently described in patients with COVID-19 compared to healthy controls. While GM-CSF might be beneficial in some circumstances as an appropriate response, in this case the inflammatory response is maladaptive by virtue of being later and disproportionate. The inhibition of GM-CSF signaling may be beneficial in improving the hyperinflammation-related lung damage in the most severe cases of COVID-19. This blockade can be achieved through antagonism of the GM-CSF receptor or the direct binding of circulating GM-CSF. Initial findings from patients with COVID-19 treated with a single intravenous dose of mavrilimumab, a monoclonal antibody binding GM-CSF receptor α, showed oxygenation improvement and shorter hospitalization. Prospective, randomized, placebo-controlled trials are ongoing. Anti-GM-CSF monoclonal antibodies, TJ003234 and gimsilumab, will be tested in clinical trials in patients with COVID-19, while lenzilumab received FDA approval for compassionate use. These trials will help inform whether blunting the inflammatory signaling provided by the GM-CSF axis in COVID-19 is beneficial.
Keywords: COVID-19; GM-CSF; IL-6; SARS-CoV-2; cytokine release syndrome; mavrilimumab.
Copyright © 2020 Bonaventura, Vecchié, Wang, Lee, Cremer, Carey, Rajendram, Hudock, Korbee, Van Tassell, Dagna and Abbate.
Figures
Similar articles
-
Therapeutic blockade of granulocyte macrophage colony-stimulating factor in COVID-19-associated hyperinflammation: challenges and opportunities.Lancet Respir Med. 2020 Aug;8(8):822-830. doi: 10.1016/S2213-2600(20)30267-8. Epub 2020 Jun 16. Lancet Respir Med. 2020. PMID: 32559419 Free PMC article. Review.
-
The Society for Immunotherapy of Cancer perspective on regulation of interleukin-6 signaling in COVID-19-related systemic inflammatory response.J Immunother Cancer. 2020 May;8(1):e000930. doi: 10.1136/jitc-2020-000930. J Immunother Cancer. 2020. PMID: 32385146 Free PMC article.
-
Case report: use of lenzilumab and tocilizumab for the treatment of coronavirus disease 2019.Immunotherapy. 2020 Oct;12(15):1121-1126. doi: 10.2217/imt-2020-0136. Epub 2020 Jun 17. Immunotherapy. 2020. PMID: 32546029 Free PMC article.
-
Blockade of GM-CSF pathway induced sustained suppression of myeloid and T cell activities in rheumatoid arthritis.Rheumatology (Oxford). 2018 Jan 1;57(1):175-184. doi: 10.1093/rheumatology/kex383. Rheumatology (Oxford). 2018. PMID: 29069507 Clinical Trial.
-
GM-CSF-based treatments in COVID-19: reconciling opposing therapeutic approaches.Nat Rev Immunol. 2020 Aug;20(8):507-514. doi: 10.1038/s41577-020-0357-7. Epub 2020 Jun 23. Nat Rev Immunol. 2020. PMID: 32576980 Free PMC article. Review.
Cited by
-
SARS-CoV-2: Recent Variants and Clinical Efficacy of Antibody-Based Therapy.Front Cell Infect Microbiol. 2022 Feb 14;12:839170. doi: 10.3389/fcimb.2022.839170. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35237535 Free PMC article. Review.
-
The Role of Cytokines and Chemokines in Severe Acute Respiratory Syndrome Coronavirus 2 Infections.Front Immunol. 2022 Apr 7;13:832394. doi: 10.3389/fimmu.2022.832394. eCollection 2022. Front Immunol. 2022. PMID: 35464491 Free PMC article. Review.
-
The pre-induction temperature affects recombinant HuGM-CSF aggregation in thermoinducible Escherichia coli.Appl Microbiol Biotechnol. 2022 Apr;106(8):2883-2902. doi: 10.1007/s00253-022-11908-z. Epub 2022 Apr 12. Appl Microbiol Biotechnol. 2022. PMID: 35412129 Free PMC article.
-
Potential therapeutic options for COVID-19: an update on current evidence.Eur J Med Res. 2022 Jan 13;27(1):6. doi: 10.1186/s40001-021-00626-3. Eur J Med Res. 2022. PMID: 35027080 Free PMC article. Review.
-
Recent advances in antibody-based immunotherapy strategies for COVID-19.J Cell Biochem. 2021 Oct;122(10):1389-1412. doi: 10.1002/jcb.30017. Epub 2021 Jun 23. J Cell Biochem. 2021. PMID: 34160093 Free PMC article. Review.
References
-
- Bo Z, Jianqing S, Yadan W, Xiancang M. Utility of Ferritin, Procalcitonin, and C-reactive Protein in Severe Patients with 2019 Novel Coronavirus Disease. (2020). Available online at: https://www.researchsquare.com/article/rs-18079/v1 (accessed June 22, 2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous