

Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis
- PMID: 32430052
- PMCID: PMC7236499
- DOI: 10.1186/s13054-020-02950-2
Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis
Abstract
Background: Sepsis and septic shock remain drivers for mortality in critically ill patients. The heterogeneity of the syndrome hinders the generation of reproducible numbers on mortality risks. Consequently, mortality rates range from 15 to 56%. We aimed to update and extend the existing knowledge from meta-analyses and estimate 30- and 90-day mortality rates for sepsis and septic shock separately, stratify rates by region and study type and assess mortality rates across different sequential organ failure assessment (SOFA) scores.
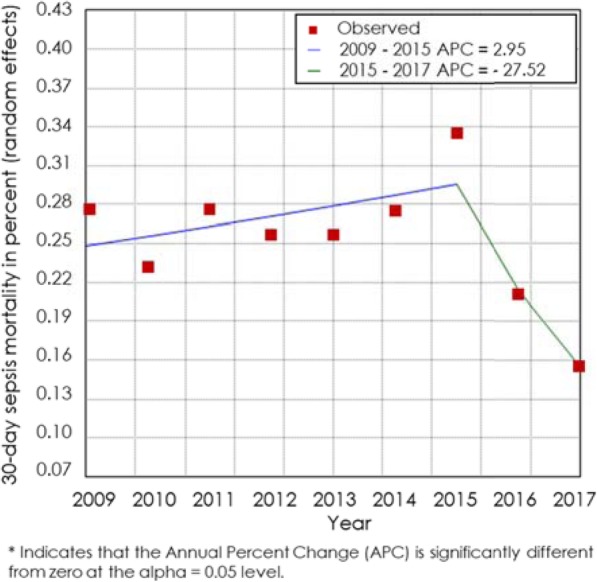
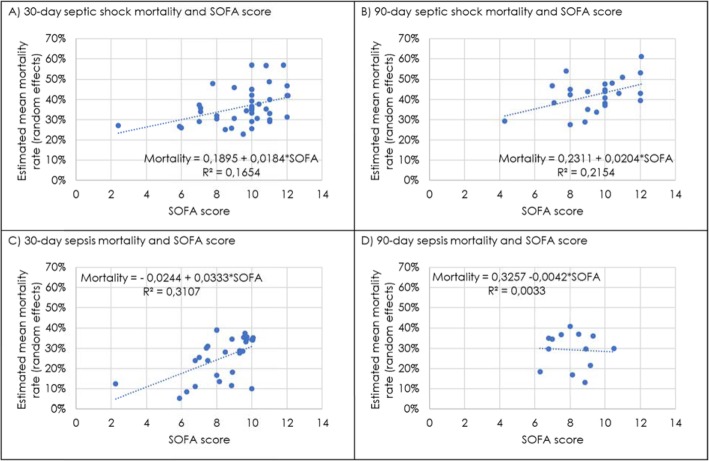
Methods: We performed a systematic review of articles published in PubMed or in the Cochrane Database, between 2009 and 2019 in English language including interventional and observational studies. A meta-analysis of pooled 28/30- and 90-day mortality rated separately for sepsis and septic shock was done using a random-effects model. Time trends were assessed via Joinpoint methodology and for the assessment of mortality rate over different SOFA scores, and linear regression was applied.
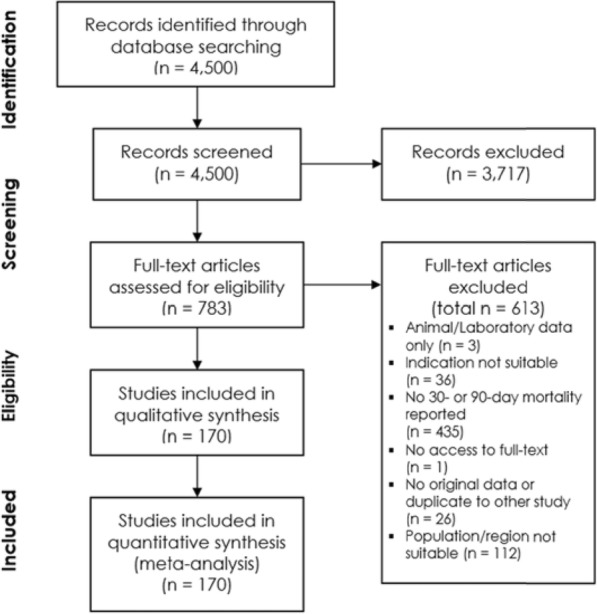
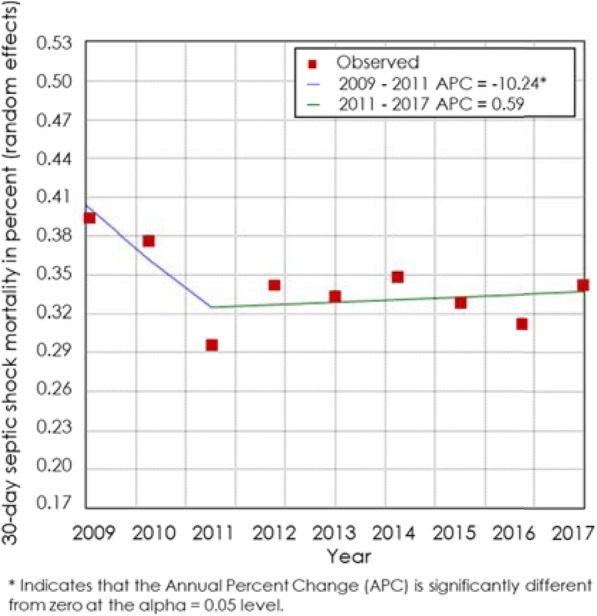
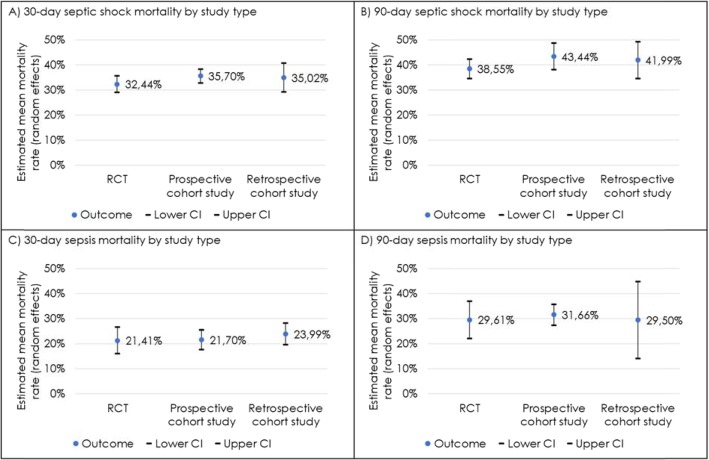
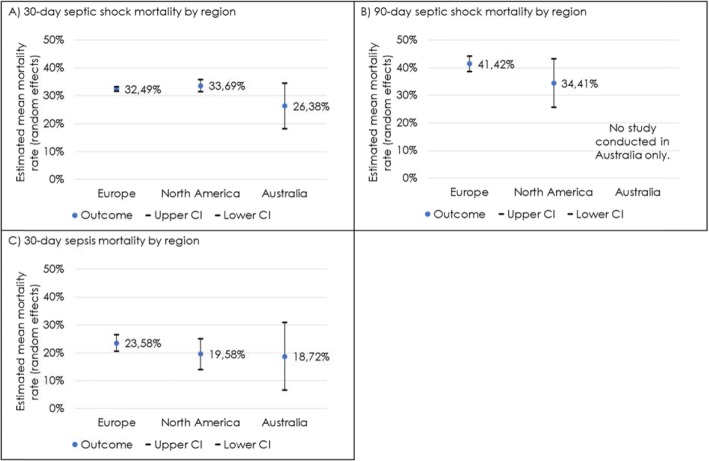
Results: Four thousand five hundred records were identified. After title/abstract screening, 783 articles were assessed in full text for eligibility. Of those, 170 studies were included. Average 30-day septic shock mortality was 34.7% (95% CI 32.6-36.9%), and 90-day septic shock mortality was 38.5% (95% CI 35.4-41.5%). Average 30-day sepsis mortality was 24.4% (95% CI 21.5-27.2%), and 90-day sepsis mortality was 32.2% (95% CI 27.0-37.5%). Estimated mortality rates from RCTs were below prospective and retrospective cohort studies. Rates varied between regions, with 30-day septic shock mortality being 33.7% (95% CI 31.5-35.9) in North America, 32.5% (95% CI 31.7-33.3) in Europe and 26.4% (95% CI 18.1-34.6) in Australia. A statistically significant decrease of 30-day septic shock mortality rate was found between 2009 and 2011, but not after 2011. Per 1-point increase of the average SOFA score, average mortality increased by 1.8-3.3%.
Conclusion: Trends of lower sepsis and continuous septic shock mortality rates over time and regional disparities indicate a remaining unmet need for improving sepsis management. Further research is needed to investigate how trends in the burden of disease influence mortality rates in sepsis and septic shock at 30- and 90-day mortality over time.
Keywords: Meta-analysis; Mortality; SOFA; Sepsis; Septic shock; Trend.
Conflict of interest statement
TV and JS are employees of LinkCare GmbH, which have received honoraria from CytoSorbents Europe GmbH. FP and DA are employees of CytoSorbents Europe GmbH.
Figures
Similar articles
-
[Mortality in sepsis and septic shock in Germany. Results of a systematic review and meta-analysis].Anaesthesist. 2021 Aug;70(8):673-680. doi: 10.1007/s00101-021-00917-8. Epub 2021 Feb 9. Anaesthesist. 2021. PMID: 33559687 Free PMC article. German.
-
Frequency and mortality of septic shock in Europe and North America: a systematic review and meta-analysis.Crit Care. 2019 May 31;23(1):196. doi: 10.1186/s13054-019-2478-6. Crit Care. 2019. PMID: 31151462 Free PMC article.
-
Global Case-Fatality Rates in Pediatric Severe Sepsis and Septic Shock: A Systematic Review and Meta-analysis.JAMA Pediatr. 2019 Apr 1;173(4):352-362. doi: 10.1001/jamapediatrics.2018.4839. JAMA Pediatr. 2019. PMID: 30742207 Free PMC article.
-
Frequency and mortality of sepsis and septic shock in China: a systematic review and meta-analysis.BMC Infect Dis. 2022 Jun 21;22(1):564. doi: 10.1186/s12879-022-07543-8. BMC Infect Dis. 2022. PMID: 35729526 Free PMC article. Review.
-
Effect of delayed antibiotic use on mortality outcomes in patients with sepsis or septic shock: A systematic review and meta-analysis.Int Immunopharmacol. 2024 Mar 10;129:111616. doi: 10.1016/j.intimp.2024.111616. Epub 2024 Feb 3. Int Immunopharmacol. 2024. PMID: 38310764 Review.
Cited by
-
Association between albumin-bilirubin score and in-hospital mortality in patients with sepsis: Evidence from two large databases.Heliyon. 2024 Jul 16;10(15):e34697. doi: 10.1016/j.heliyon.2024.e34697. eCollection 2024 Aug 15. Heliyon. 2024. PMID: 39170393 Free PMC article.
-
Deciphering the immune-metabolic nexus in sepsis: a single-cell sequencing analysis of neutrophil heterogeneity and risk stratification.Front Immunol. 2024 Jul 23;15:1398719. doi: 10.3389/fimmu.2024.1398719. eCollection 2024. Front Immunol. 2024. PMID: 39108261 Free PMC article.
-
Predictive value of neutrophil-to-lymphocyte and platelet ratio in in-hospital mortality in septic patients.Heliyon. 2022 Nov 16;8(11):e11498. doi: 10.1016/j.heliyon.2022.e11498. eCollection 2022 Nov. Heliyon. 2022. PMID: 36439769 Free PMC article.
-
Effectiveness of β-blockers in improving 28-day mortality in septic shock: insights from subgroup analysis and retrospective observational study.Front Cardiovasc Med. 2024 Sep 3;11:1438798. doi: 10.3389/fcvm.2024.1438798. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39290214 Free PMC article.
-
A simplified machine learning model utilizing platelet-related genes for predicting poor prognosis in sepsis.Front Immunol. 2023 Nov 20;14:1286203. doi: 10.3389/fimmu.2023.1286203. eCollection 2023. Front Immunol. 2023. PMID: 38054005 Free PMC article.
References
-
- WHO. Sepsis [Internet]. 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/sepsis.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
