

Kidney Disease, Race, and GFR Estimation
- PMID: 32393465
- PMCID: PMC7409747
- DOI: 10.2215/CJN.12791019
Kidney Disease, Race, and GFR Estimation
Abstract
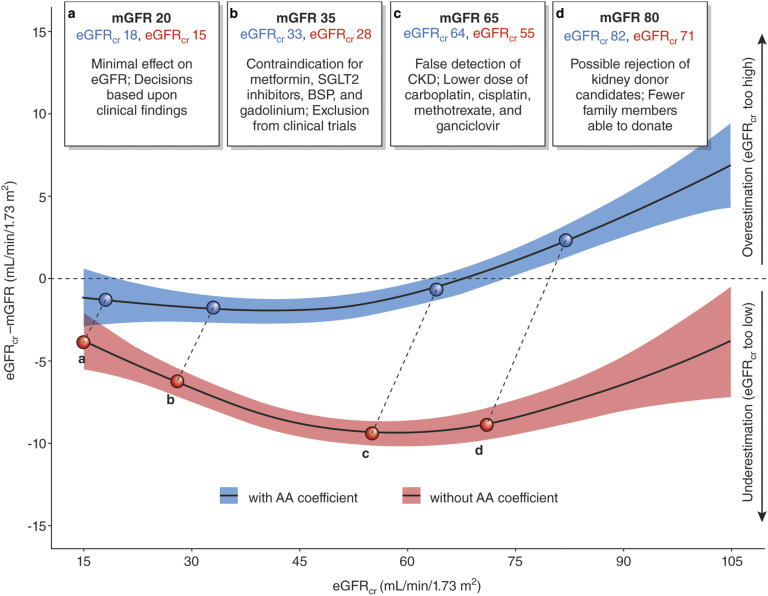
Assessment of GFR is central to clinical practice, research, and public health. Current Kidney Disease Improving Global Outcomes guidelines recommend measurement of serum creatinine to estimate GFR as the initial step in GFR evaluation. Serum creatinine is influenced by creatinine metabolism as well as GFR; hence, all equations to estimate GFR from serum creatinine include surrogates for muscle mass, such as age, sex, race, height, or weight. The guideline-recommended equation in adults (the 2009 Chronic Kidney Disease Epidemiology Collaboration creatinine equation) includes a term for race (specified as black versus nonblack), which improves the accuracy of GFR estimation by accounting for differences in non-GFR determinants of serum creatinine by race in the study populations used to develop the equation. In that study, blacks had a 16% higher average measured GFR compared with nonblacks with the same age, sex, and serum creatinine. The reasons for this difference are only partly understood, and the use of race in GFR estimation has limitations. Some have proposed eliminating the race coefficient, but this would induce a systematic underestimation of measured GFR in blacks, with potential unintended consequences at the individual and population levels. We propose a more cautious approach that maintains and improves accuracy of GFR estimates and avoids disadvantaging any racial group. We suggest full disclosure of use of race in GFR estimation, accommodation of those who decline to identify their race, and shared decision making between health care providers and patients. We also suggest mindful use of cystatin C as a confirmatory test as well as clearance measurements. It would be preferable to avoid specification of race in GFR estimation if there was a superior, evidence-based substitute. The goal of future research should be to develop more accurate methods for GFR estimation that do not require use of race or other demographic characteristics.
Keywords: African Americans; Body Weights and Measures; Chronic; Cystatin C; Decision Making; Demography; Health Personnel; Kidney Function Tests; Public Health; Renal Insufficiency; Shared; creatinine; glomerular filtration rate; human.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Precision in GFR Reporting: Let's Stop Playing the Race Card.Clin J Am Soc Nephrol. 2020 Aug 7;15(8):1201-1202. doi: 10.2215/CJN.00690120. Epub 2020 May 11. Clin J Am Soc Nephrol. 2020. PMID: 32401730 Free PMC article. No abstract available.
Similar articles
-
Cystatin C-Based Equation to Estimate GFR without the Inclusion of Race and Sex.N Engl J Med. 2023 Jan 26;388(4):333-343. doi: 10.1056/NEJMoa2203769. N Engl J Med. 2023. PMID: 36720134
-
Is the Chronic Kidney Disease Epidemiology Collaboration four-level race equation better than the cystatin C equation?Nephrology (Carlton). 2012 May;17(4):407-14. doi: 10.1111/j.1440-1797.2012.01568.x. Nephrology (Carlton). 2012. PMID: 22257305
-
Estimating glomerular filtration rate by serum creatinine or/and cystatin C equations: An analysis of multi-centre Chinese subjects.Nephrology (Carlton). 2016 May;21(5):372-8. doi: 10.1111/nep.12636. Nephrology (Carlton). 2016. PMID: 26427030
-
A Unifying Approach for GFR Estimation: Recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease.Am J Kidney Dis. 2022 Feb;79(2):268-288.e1. doi: 10.1053/j.ajkd.2021.08.003. Epub 2021 Sep 23. Am J Kidney Dis. 2022. PMID: 34563581 Review.
-
Calibration and precision of serum creatinine and plasma cystatin C measurement: impact on the estimation of glomerular filtration rate.J Nephrol. 2014 Oct;27(5):467-75. doi: 10.1007/s40620-014-0087-7. Epub 2014 Apr 8. J Nephrol. 2014. PMID: 24711159 Review.
Cited by
-
Reassessing the Inclusion of Race in Diagnosing Kidney Diseases: An Interim Report From the NKF-ASN Task Force.Am J Kidney Dis. 2021 Jul;78(1):103-115. doi: 10.1053/j.ajkd.2021.03.008. Epub 2021 Apr 9. Am J Kidney Dis. 2021. PMID: 33845065 Free PMC article.
-
An endo-functionalized molecular cage for selective potentiometric determination of creatinine.Chem Sci. 2024 Aug 22;15(36):14791-7. doi: 10.1039/d4sc04950k. Online ahead of print. Chem Sci. 2024. PMID: 39184288 Free PMC article.
-
Demographic and clinical profile of black patients with chronic kidney disease attending a tertiary hospital in Johannesburg, South Africa.PLoS One. 2022 Sep 19;17(9):e0266155. doi: 10.1371/journal.pone.0266155. eCollection 2022. PLoS One. 2022. PMID: 36121812 Free PMC article.
-
Recommendations to advance digital health equity: a systematic review of qualitative studies.NPJ Digit Med. 2024 Jun 29;7(1):173. doi: 10.1038/s41746-024-01177-7. NPJ Digit Med. 2024. PMID: 38951666 Free PMC article. Review.
-
Development of a multimodal kidney age prediction based on automatic segmentation CT image in patients with normal renal function.Clin Kidney J. 2023 Jul 19;16(11):2091-2099. doi: 10.1093/ckj/sfad167. eCollection 2023 Nov. Clin Kidney J. 2023. PMID: 37915907 Free PMC article.
References
-
- Levey AS, Coresh J, Tighiouart H, Greene T, Inker LA: Strengths and limitations of estimated and measured GFR. Nat Rev Nephrol 15: 784, 2019. - PubMed
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators : Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 392: 1789–1858, 2018. - PMC - PubMed
-
- Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, Saran R, Wang AY, Yang CW: Chronic kidney disease: Global dimension and perspectives. Lancet 382: 260–272, 2013. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
