

Optimal individualized decision rules from a multi-arm trial: A comparison of methods and an application to tailoring inter-donation intervals among blood donors in the UK
- PMID: 32380893
- PMCID: PMC7682530
- DOI: 10.1177/0962280220920669
Optimal individualized decision rules from a multi-arm trial: A comparison of methods and an application to tailoring inter-donation intervals among blood donors in the UK
Abstract
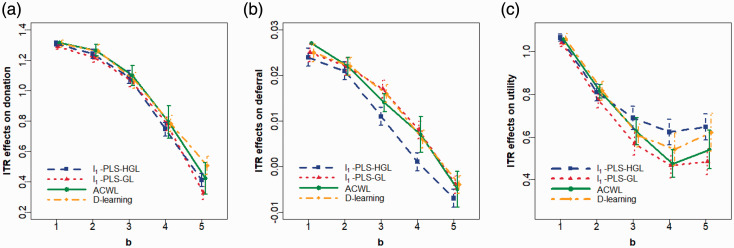
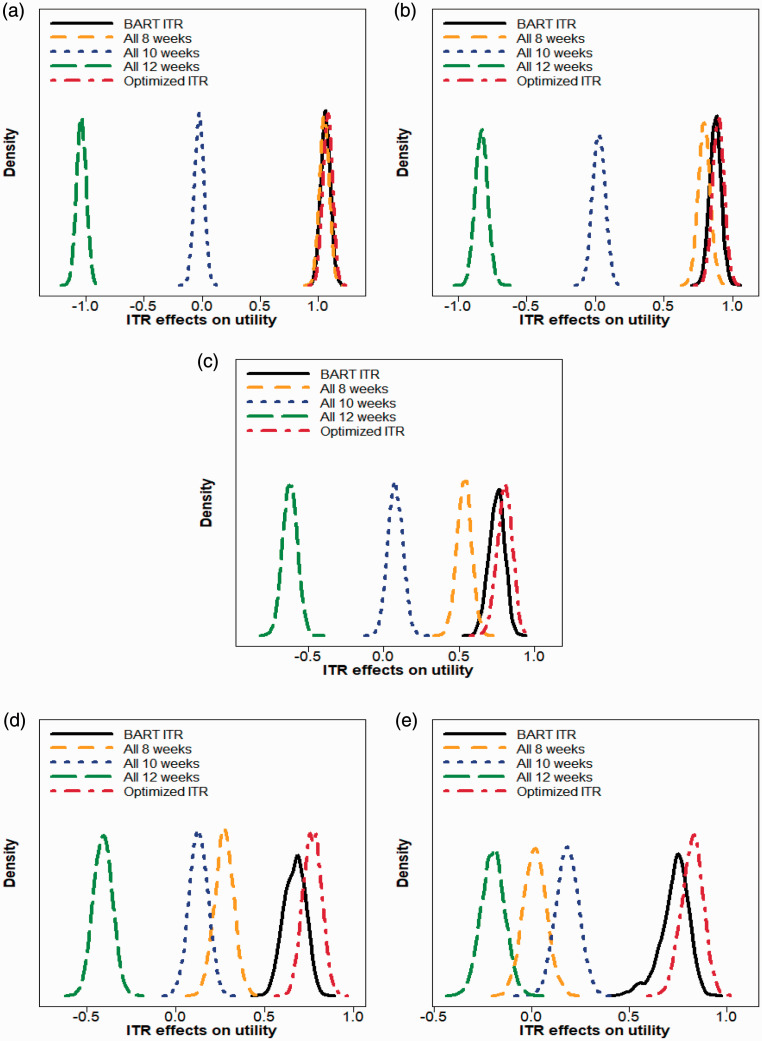
There is a growing interest in precision medicine where individual heterogeneity is incorporated into decision-making and treatments are tailored to individuals to provide better healthcare. One important aspect of precision medicine is the estimation of the optimal individualized treatment rule (ITR) that optimizes the expected outcome. Most methods developed for this purpose are restricted to the setting with two treatments, while clinical studies with more than two treatments are common in practice. In this work, we summarize methods to estimate the optimal ITR in the multi-arm setting and compare their performance in large-scale clinical trials via simulation studies. We then illustrate their utilities with a case study using the data from the INTERVAL trial, which randomly assigned over 20,000 male blood donors from England to one of the three inter-donation intervals (12-week, 10-week, and eight-week) over two years. We estimate the optimal individualized donation strategies under three different objectives. Our findings are fairly consistent across five different approaches that are applied: when we target the maximization of the total units of blood collected, almost all donors are assigned to the eight-week inter-donation interval, whereas if we aim at minimizing the low hemoglobin deferral rates, almost all donors are assigned to donate every 12 weeks. However, when the goal is to maximize the utility score that "discounts" the total units of blood collected by the incidences of low hemoglobin deferrals, we observe some heterogeneity in the optimal inter-donation interval across donors and the optimal donor assignment strategy is highly dependent on the trade-off parameter in the utility function.
Keywords: Precision medicine; blood donation; individualized treatment rule; multi-arm trial; utility function.
Figures
Similar articles
-
Longer-term efficiency and safety of increasing the frequency of whole blood donation (INTERVAL): extension study of a randomised trial of 20 757 blood donors.Lancet Haematol. 2019 Oct;6(10):e510-e520. doi: 10.1016/S2352-3026(19)30106-1. Epub 2019 Aug 2. Lancet Haematol. 2019. PMID: 31383583 Free PMC article. Clinical Trial.
-
Efficiency and safety of varying the frequency of whole blood donation (INTERVAL): a randomised trial of 45 000 donors.Lancet. 2017 Nov 25;390(10110):2360-2371. doi: 10.1016/S0140-6736(17)31928-1. Epub 2017 Sep 21. Lancet. 2017. PMID: 28941948 Free PMC article. Clinical Trial.
-
The INTERVAL trial to determine whether intervals between blood donations can be safely and acceptably decreased to optimise blood supply: study protocol for a randomised controlled trial.Trials. 2014 Sep 17;15:363. doi: 10.1186/1745-6215-15-363. Trials. 2014. PMID: 25230735 Free PMC article. Clinical Trial.
-
Options for possible changes to the blood donation service: health economics modelling.Southampton (UK): NIHR Journals Library; 2018 Dec. Southampton (UK): NIHR Journals Library; 2018 Dec. PMID: 30540399 Free Books & Documents. Review.
-
Evidence-based criteria for the care and selection of blood donors, with some comments on the relationship to blood supply, and emphasis on the management of donation-induced iron depletion.Transfus Med. 2008 Feb;18(1):13-27. doi: 10.1111/j.1365-3148.2007.00818.x. Transfus Med. 2008. PMID: 18279189 Review.
Cited by
-
Using the Causal Inference Framework to Support Individualized Drug Treatment Decisions Based on Observational Healthcare Data.Clin Epidemiol. 2020 Nov 2;12:1223-1234. doi: 10.2147/CLEP.S274466. eCollection 2020. Clin Epidemiol. 2020. PMID: 33173350 Free PMC article.
-
Optimal Donor Selection for Hematopoietic Cell Transplantation Using Bayesian Machine Learning.JCO Clin Cancer Inform. 2021 May;5:494-507. doi: 10.1200/CCI.20.00185. JCO Clin Cancer Inform. 2021. PMID: 33950708 Free PMC article.
References
-
- Lipkovich I, Dmitrienko A, BD’AgostinoR. Tutorial in biostatistics: data-driven subgroup identification and analysis in clinical trials. Stat Med 2017; 36: 136–196. - PubMed
-
- Lou Z, Shao J, Yu M. Optimal treatment assignment to maximize expected outcome with multiple treatments. Biometrics 2018; 74: 506–516. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
