

Effect of Combined Immune Checkpoint Inhibition vs Best Supportive Care Alone in Patients With Advanced Colorectal Cancer: The Canadian Cancer Trials Group CO.26 Study
- PMID: 32379280
- PMCID: PMC7206536
- DOI: 10.1001/jamaoncol.2020.0910
Effect of Combined Immune Checkpoint Inhibition vs Best Supportive Care Alone in Patients With Advanced Colorectal Cancer: The Canadian Cancer Trials Group CO.26 Study
Abstract
Importance: Single-agent immune checkpoint inhibition has not shown activities in advanced refractory colorectal cancer (CRC), other than in those patients who are microsatellite-instability high (MSI-H).
Objective: To evaluate whether combining programmed death-ligand 1 (PD-L1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibition improved patient survival in metastatic refractory CRC.
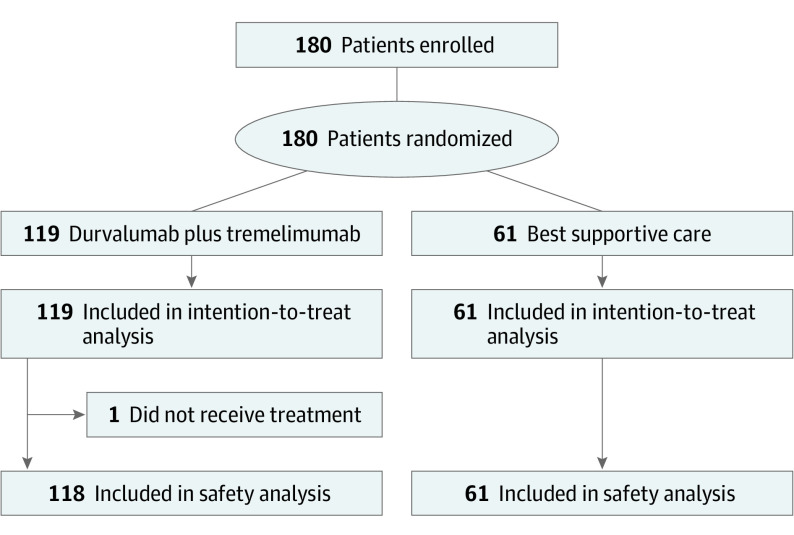
Design, setting, and participants: A randomized phase 2 study was conducted in 27 cancer centers across Canada between August 2016 and June 2017, and data were analyzed on October 18, 2018. Eligible patients had histologically confirmed adenocarcinoma of the colon or rectum; received all available standard systemic therapies (fluoropyrimidines, oxaliplatin, irinotecan, and bevacizumab if appropriate; cetuximab or panitumumab if RAS wild-type tumors; regorafenib if available); were aged 18 years or older; had adequate organ function; had Eastern Cooperative Oncology Group performance status of 0 or 1, and measurable disease.
Interventions: We randomly assigned patients to receive either 75 mg of tremelimumab every 28 days for the first 4 cycles plus 1500 mg durvalumab every 28 days, or best supportive care alone (BSC) in a 2:1 ratio.
Main outcomes and measures: The primary end point was overall survival (OS) and a 2-sided P<.10 was considered statistically significant. Circulating cell-free DNA from baseline plasma was used to determine microsatellite instability (MSI) and tumor mutation burden (TMB).
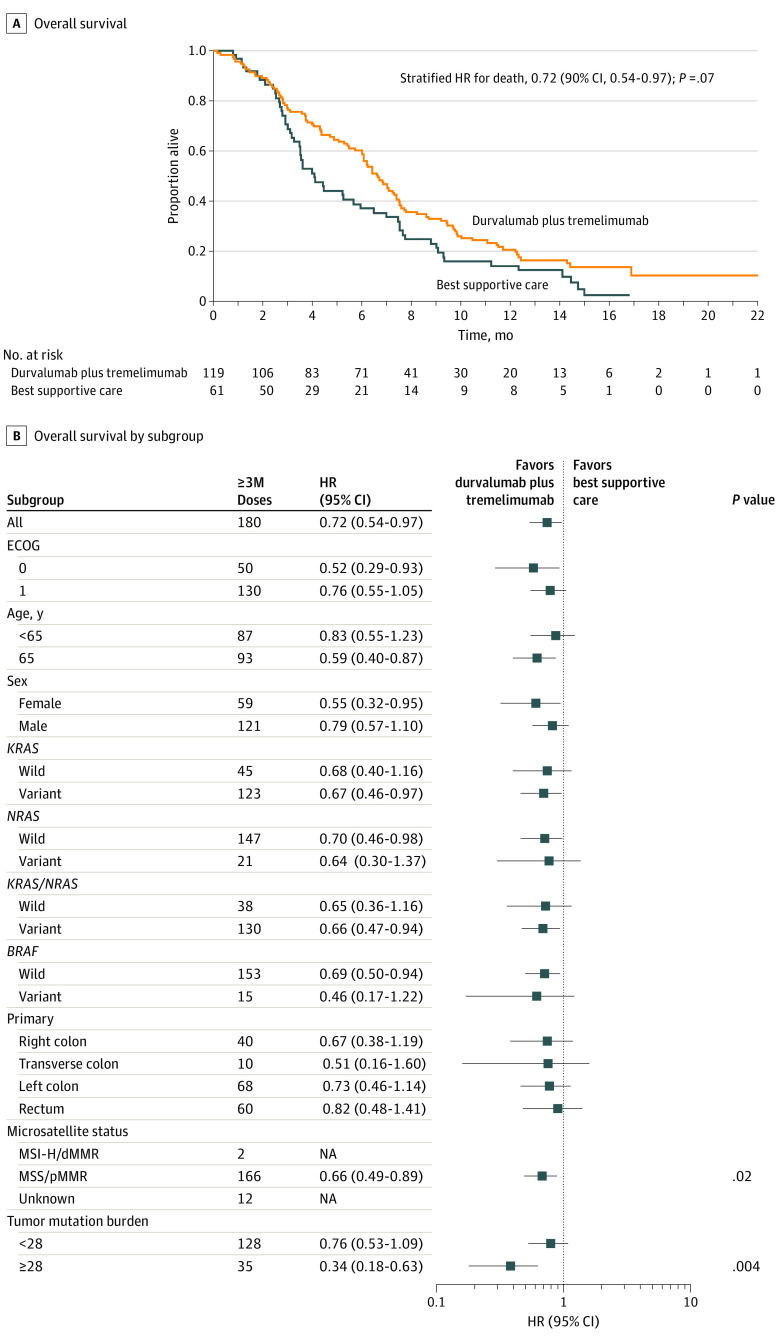
Results: Of 180 patients enrolled (121 men [67.2%] and 59 women [32.8%]; median [range] age, 65 [36-87] years), 179 were treated. With a median follow-up of 15.2 months, the median OS was 6.6 months for durvalumab and tremelimumab and 4.1 months for BSC (hazard ratio [HR], 0.72; 90% CI, 0.54-0.97; P = .07). Progression-free survival was 1.8 months and 1.9 months respectively (HR, 1.01; 90% CI, 0.76-1.34). Grade 3 or 4 adverse events were significantly more frequent with immunotherapy (75 [64%] patients in the treatment group had at least 1 grade 3 or higher adverse event vs 12 [20%] in the BSC group). Circulating cell-free DNA analysis was successful in 168 of 169 patients with available samples. In patients who were microsatellite stable (MSS), OS was significantly improved with durvalumab and tremelimumab (HR, 0.66; 90% CI, 0.49-0.89; P = .02). Patients who were MSS with plasma TMB of 28 variants per megabase or more (21% of MSS patients) had the greatest OS benefit (HR, 0.34; 90% CI, 0.18-0.63; P = .004).
Conclusions and relevance: This phase 2 study suggests that combined immune checkpoint inhibition with durvalumab plus tremelimumab may be associated with prolonged OS in patients with advanced refractory CRC. Elevated plasma TMB may select patients most likely to benefit from durvalumab and tremelimumab. Further confirmation studies are warranted.
Trial registration: ClinicalTrials.gov Identifier: NCT02870920.
Conflict of interest statement
Figures
Comment in
-
Efficacy of Immunotherapy in Microsatellite-Stable or Mismatch Repair Proficient Colorectal Cancer-Fact or Fiction?JAMA Oncol. 2020 Jun 1;6(6):823-824. doi: 10.1001/jamaoncol.2020.0504. JAMA Oncol. 2020. PMID: 32379270 No abstract available.
Similar articles
-
Durvalumab With or Without Tremelimumab vs Standard Chemotherapy in First-line Treatment of Metastatic Non-Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial.JAMA Oncol. 2020 May 1;6(5):661-674. doi: 10.1001/jamaoncol.2020.0237. JAMA Oncol. 2020. PMID: 32271377 Free PMC article. Clinical Trial.
-
Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (DANUBE): a randomised, open-label, multicentre, phase 3 trial.Lancet Oncol. 2020 Dec;21(12):1574-1588. doi: 10.1016/S1470-2045(20)30541-6. Epub 2020 Sep 21. Lancet Oncol. 2020. PMID: 32971005 Clinical Trial.
-
Durvalumab plus tremelimumab alone or in combination with low-dose or hypofractionated radiotherapy in metastatic non-small-cell lung cancer refractory to previous PD(L)-1 therapy: an open-label, multicentre, randomised, phase 2 trial.Lancet Oncol. 2022 Feb;23(2):279-291. doi: 10.1016/S1470-2045(21)00658-6. Epub 2022 Jan 13. Lancet Oncol. 2022. PMID: 35033226 Free PMC article. Clinical Trial.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article. Review.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.Health Technol Assess. 2007 Mar;11(12):1-128, iii-iv. doi: 10.3310/hta11120. Health Technol Assess. 2007. PMID: 17346499 Review.
Cited by
-
Are Molecular Alterations Linked to Genetic Instability Worth to Be Included as Biomarkers for Directing or Excluding Melanoma Patients to Immunotherapy?Front Oncol. 2021 May 5;11:666624. doi: 10.3389/fonc.2021.666624. eCollection 2021. Front Oncol. 2021. PMID: 34026645 Free PMC article. Review.
-
Targeting CTLA-4: a possible solution for microsatellite-stable colorectal cancer.Genes Immun. 2023 Dec;24(6):283-284. doi: 10.1038/s41435-023-00223-w. Epub 2023 Dec 8. Genes Immun. 2023. PMID: 38066340
-
Tumor-associated mesenchymal stromal cells modulate macrophage phagocytosis in stromal-rich colorectal cancer via PD-1 signaling.iScience. 2024 Aug 22;27(9):110701. doi: 10.1016/j.isci.2024.110701. eCollection 2024 Sep 20. iScience. 2024. PMID: 39310770 Free PMC article.
-
Recent developments in immunotherapy for gastrointestinal tract cancers.J Hematol Oncol. 2024 Aug 9;17(1):65. doi: 10.1186/s13045-024-01578-x. J Hematol Oncol. 2024. PMID: 39123202 Free PMC article. Review.
-
Immunocheckpoint Inhibitors in Microsatellite-Stable or Proficient Mismatch Repair Metastatic Colorectal Cancer: Are We Entering a New Era?Cancers (Basel). 2023 Oct 28;15(21):5189. doi: 10.3390/cancers15215189. Cancers (Basel). 2023. PMID: 37958363 Free PMC article. Review.
References
-
- Venook AP, Niedzwiecki D, Lenz HJ, et al. . Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced or metastatic colorectal cancer: a randomized clinical trial. JAMA. 2017;317(23):2392-2401. doi:10.1001/jama.2017.7105 - DOI - PMC - PubMed
-
- Stintzing S, Modest DP, Rossius L, et al. ; FIRE-3 investigators . FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab for metastatic colorectal cancer (FIRE-3): a post-hoc analysis of tumour dynamics in the final RAS wild-type subgroup of this randomised open-label phase 3 trial. Lancet Oncol. 2016;17(10):1426-1434. doi:10.1016/S1470-2045(16)30269-8 - DOI - PubMed
-
- Grothey A, Van Cutsem E, Sobrero A, et al. ; CORRECT Study Group . Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013;381(9863):303-312. doi:10.1016/S0140-6736(12)61900-X - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
