

CO-RADS: A Categorical CT Assessment Scheme for Patients Suspected of Having COVID-19-Definition and Evaluation
- PMID: 32339082
- PMCID: PMC7233402
- DOI: 10.1148/radiol.2020201473
CO-RADS: A Categorical CT Assessment Scheme for Patients Suspected of Having COVID-19-Definition and Evaluation
Abstract
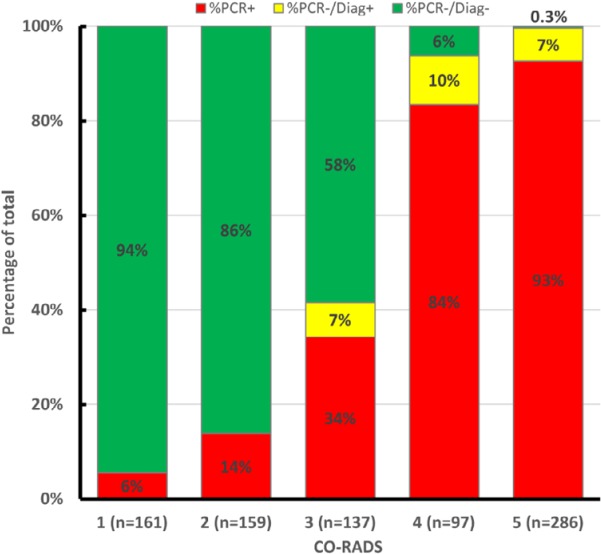
Background A categorical CT assessment scheme for suspicion of pulmonary involvement of coronavirus disease 2019 (COVID-19 provides a basis for gathering scientific evidence and improved communication with referring physicians. Purpose To introduce the COVID-19 Reporting and Data System (CO-RADS) for use in the standardized assessment of pulmonary involvement of COVID-19 on unenhanced chest CT images and to report its initial interobserver agreement and performance. Materials and Methods The Dutch Radiological Society developed CO-RADS based on other efforts for standardization, such as the Lung Imaging Reporting and Data System or Breast Imaging Reporting and Data System. CO-RADS assesses the suspicion for pulmonary involvement of COVID-19 on a scale from 1 (very low) to 5 (very high). The system is meant to be used in patients with moderate to severe symptoms of COVID-19. The system was evaluated by using 105 chest CT scans of patients admitted to the hospital with clinical suspicion of COVID-19 and in whom reverse transcription-polymerase chain reaction (RT-PCR) was performed (mean, 62 years ± 16 [standard deviation]; 61 men, 53 with positive RT-PCR results). Eight observers used CO-RADS to assess the scans. Fleiss κ value was calculated, and scores of individual observers were compared with the median of the remaining seven observers. The resulting area under the receiver operating characteristics curve (AUC) was compared with results from RT-PCR and clinical diagnosis of COVID-19. Results There was absolute agreement among observers in 573 (68.2%) of 840 observations. Fleiss κ value was 0.47 (95% confidence interval [CI]: 0.45, 0.47), with the highest κ value for CO-RADS categories 1 (0.58, 95% CI: 0.54, 0.62) and 5 (0.68, 95% CI: 0.65, 0.72). The average AUC was 0.91 (95% CI: 0.85, 0.97) for predicting RT-PCR outcome and 0.95 (95% CI: 0.91, 0.99) for clinical diagnosis. The false-negative rate for CO-RADS 1 was nine of 161 cases (5.6%; 95% CI: 1.0%, 10%), and the false-positive rate for CO-RADS category 5 was one of 286 (0.3%; 95% CI: 0%, 1.0%). Conclusion The coronavirus disease 2019 (COVID-19) Reporting and Data System (CO-RADS) is a categorical assessment scheme for pulmonary involvement of COVID-19 at unenhanced chest CT that performs very well in predicting COVID-19 in patients with moderate to severe symptoms and has substantial interobserver agreement, especially for categories 1 and 5. © RSNA, 2020 Online supplemental material is available for this article.
Figures
Comment in
-
Extensive pulmonary perfusion defects compatible with microthrombosis and thromboembolic disease in severe Covid-19 pneumonia.Thromb Res. 2020 Dec;196:135-137. doi: 10.1016/j.thromres.2020.08.026. Epub 2020 Aug 22. Thromb Res. 2020. PMID: 32866825 Free PMC article. No abstract available.
Similar articles
-
Chest CT in the Emergency Department for Diagnosis of COVID-19 Pneumonia: Dutch Experience.Radiology. 2021 Feb;298(2):E98-E106. doi: 10.1148/radiol.2020203465. Epub 2020 Nov 17. Radiology. 2021. PMID: 33201791 Free PMC article.
-
Diagnostic accuracy and interobserver variability of CO-RADS in patients with suspected coronavirus disease-2019: a multireader validation study.Eur Radiol. 2021 Apr;31(4):1932-1940. doi: 10.1007/s00330-020-07273-y. Epub 2020 Sep 23. Eur Radiol. 2021. PMID: 32968883 Free PMC article.
-
Radiological Society of North America (RSNA) Expert Consensus Statement Related to Chest CT Findings in COVID-19 Versus CO-RADS: Comparison of Reporting System Performance Among Chest Radiologists and End-User Preference.Can Assoc Radiol J. 2021 Nov;72(4):806-813. doi: 10.1177/0846537120968919. Epub 2020 Nov 3. Can Assoc Radiol J. 2021. PMID: 33138634
-
[Radiological manifestations of pulmonary diseases in COVID-19].Radiologe. 2020 Oct;60(10):908-915. doi: 10.1007/s00117-020-00749-4. Radiologe. 2020. PMID: 32897438 Free PMC article. Review. German.
-
The role of iodinated contrast media in computed tomography structured Reporting and Data Systems (RADS): a narrative review.Quant Imaging Med Surg. 2023 Nov 1;13(11):7621-7631. doi: 10.21037/qims-23-603. Epub 2023 Aug 16. Quant Imaging Med Surg. 2023. PMID: 37969632 Free PMC article. Review.
Cited by
-
Clinical and computed tomography features of patients suspected of COVID-19 in the university hospital of Oran, Algeria.Tunis Med. 2022 mai;100(5):374-383. Tunis Med. 2022. PMID: 36206086 Free PMC article. English.
-
A reporting and analysis framework for structured evaluation of COVID-19 clinical and imaging data.NPJ Digit Med. 2021 Apr 12;4(1):69. doi: 10.1038/s41746-021-00439-y. NPJ Digit Med. 2021. PMID: 33846548 Free PMC article.
-
Radiographers and COVID-19 pneumonia: Diagnostic performance using CO-RADS.Radiography (Lond). 2021 Nov;27(4):1078-1084. doi: 10.1016/j.radi.2021.04.010. Epub 2021 Apr 30. Radiography (Lond). 2021. PMID: 33975783 Free PMC article.
-
Automated diagnosis of COVID-19 using radiological modalities and Artificial Intelligence functionalities: A retrospective study based on chest HRCT database.Biomed Signal Process Control. 2023 Feb;80:104297. doi: 10.1016/j.bspc.2022.104297. Epub 2022 Oct 18. Biomed Signal Process Control. 2023. PMID: 36275840 Free PMC article.
-
How accurate are radiography and computed tomography in the diagnosis of COVID-19?-A Bayesian approach.Acta Radiol Open. 2022 Nov 24;11(11):20584601221142256. doi: 10.1177/20584601221142256. eCollection 2022 Nov. Acta Radiol Open. 2022. PMID: 36447453 Free PMC article.
References
-
- Li Y, Yao L, Li J, et al. . Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19. J Med Virol. 2020;http://doi.wiley.com/10.1002/jmv.25786. Accessed April 15, 2020. - DOI - PMC - PubMed
-
- Wang W, Xu Y, Gao R, et al. . Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA. 2020;https://jamanetwork.com/journals/jama/fullarticle/2762997. Accessed April 15, 2020. - PMC - PubMed
-
- Corman VM, Landt O, Kaiser M, et al. . Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance. 2020;25(3); https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.3..... Accessed April 16, 2020. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
