

COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review
- PMID: 32311448
- PMCID: PMC7164881
- DOI: 10.1016/j.jacc.2020.04.031
COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review
Abstract
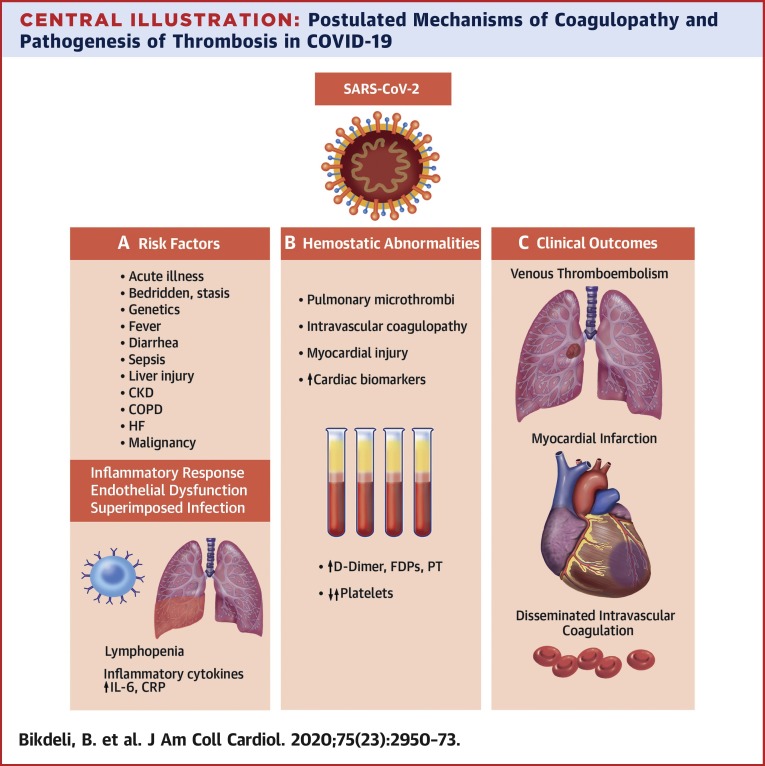
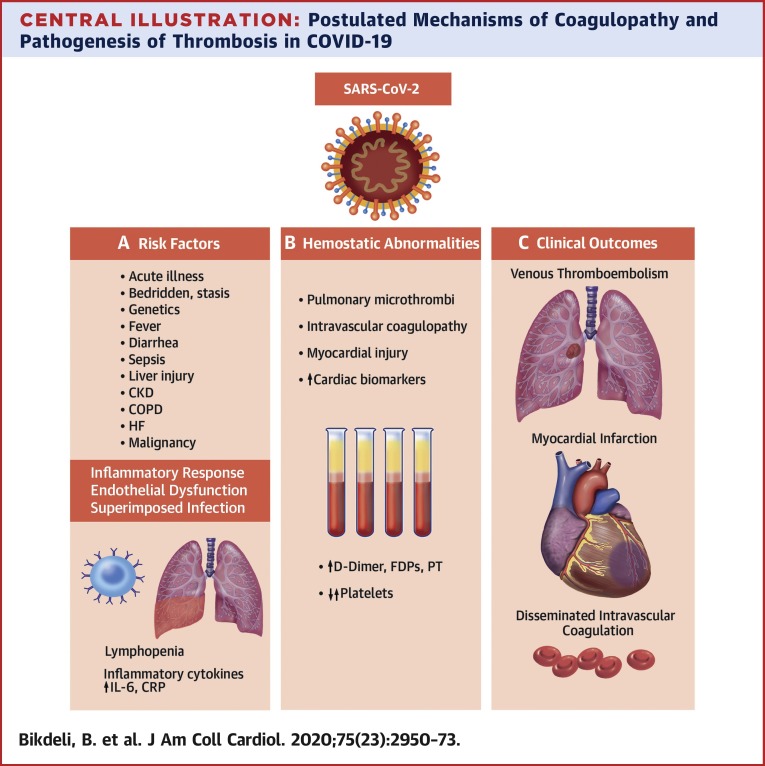
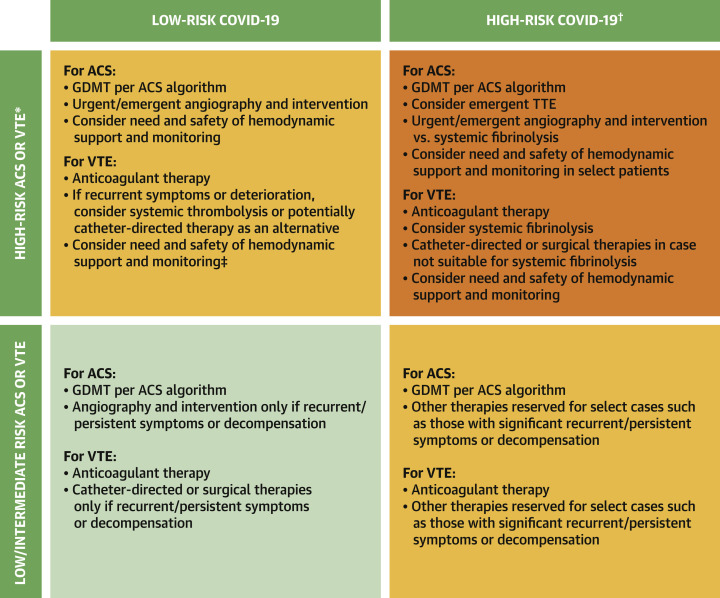
Coronavirus disease-2019 (COVID-19), a viral respiratory illness caused by the severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2), may predispose patients to thrombotic disease, both in the venous and arterial circulations, because of excessive inflammation, platelet activation, endothelial dysfunction, and stasis. In addition, many patients receiving antithrombotic therapy for thrombotic disease may develop COVID-19, which can have implications for choice, dosing, and laboratory monitoring of antithrombotic therapy. Moreover, during a time with much focus on COVID-19, it is critical to consider how to optimize the available technology to care for patients without COVID-19 who have thrombotic disease. Herein, the authors review the current understanding of the pathogenesis, epidemiology, management, and outcomes of patients with COVID-19 who develop venous or arterial thrombosis, of those with pre-existing thrombotic disease who develop COVID-19, or those who need prevention or care for their thrombotic disease during the COVID-19 pandemic.
Keywords: COVID-19; SARS-CoV-2; anticoagulant; antiplatelet; antithrombotic therapy; thrombosis.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Rescue fibrinolysis in suspected massive pulmonary embolism during SARS-CoV-2 pandemic.Resuscitation. 2020 Jul;152:86-88. doi: 10.1016/j.resuscitation.2020.05.020. Epub 2020 May 20. Resuscitation. 2020. PMID: 32445784 Free PMC article. No abstract available.
-
Spontaneous coronavirus disease 2019 (COVID-19)-associated luminal aortic thrombus.J Thorac Cardiovasc Surg. 2020 Aug;160(2):e13-e14. doi: 10.1016/j.jtcvs.2020.05.024. Epub 2020 Jun 9. J Thorac Cardiovasc Surg. 2020. PMID: 32534745 Free PMC article. No abstract available.
-
COVID-19 and venous thromboembolism: part of a multisystem disease.Rev Esp Enferm Dig. 2021 May;113(5):390. doi: 10.17235/reed.2021.7907/2021. Rev Esp Enferm Dig. 2021. PMID: 33733807
Similar articles
-
[COVID-19 and thromboprophylaxis: Recommendations for our clinical practice in Primary Care].Semergen. 2020 Oct;46(7):479-486. doi: 10.1016/j.semerg.2020.07.007. Epub 2020 Sep 18. Semergen. 2020. PMID: 33046353 Free PMC article. Spanish.
-
SEDAR-SEMICYUC consensus recommendations on the management of haemostasis disorders in severely ill patients with COVID-19 infection.Rev Esp Anestesiol Reanim (Engl Ed). 2020 Aug-Sep;67(7):391-399. doi: 10.1016/j.redar.2020.05.007. Epub 2020 May 23. Rev Esp Anestesiol Reanim (Engl Ed). 2020. PMID: 32591185 Free PMC article. English, Spanish.
-
The Emerging Threat of (Micro)Thrombosis in COVID-19 and Its Therapeutic Implications.Circ Res. 2020 Jul 31;127(4):571-587. doi: 10.1161/CIRCRESAHA.120.317447. Epub 2020 Jun 26. Circ Res. 2020. PMID: 32586214 Free PMC article. Review.
-
Viral Coagulopathy in Patients With COVID-19: Treatment and Care.Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620936776. doi: 10.1177/1076029620936776. Clin Appl Thromb Hemost. 2020. PMID: 32687449 Free PMC article. Review.
-
COVID-19-associated coagulopathy.Diagnosis (Berl). 2020 Nov 18;7(4):357-363. doi: 10.1515/dx-2020-0078. Diagnosis (Berl). 2020. PMID: 32683333 Review.
Cited by
-
Correlation of Coagulation Parameters With Clinical Outcomes During the Coronavirus-19 Surge in New York: Observational Cohort.Front Physiol. 2021 Feb 23;12:618929. doi: 10.3389/fphys.2021.618929. eCollection 2021. Front Physiol. 2021. PMID: 33708136 Free PMC article.
-
Endothelial cell, myeloid, and adaptive immune responses in SARS-CoV-2 infection.FASEB J. 2021 May;35(5):e21577. doi: 10.1096/fj.202100024R. FASEB J. 2021. PMID: 33831263 Free PMC article. Review.
-
Acute inflammatory demyelinating polyneuropathy or Guillain-Barré syndrome associated with COVID-19: a case report.J Med Case Rep. 2021 Apr 28;15(1):219. doi: 10.1186/s13256-021-02831-4. J Med Case Rep. 2021. PMID: 33910640 Free PMC article.
-
Knowledge Gaps for Prophylactic Use of Antithrombotic Agents in Patients with COVID-19: Insights into New SARS-CoV-2 Variants, Vaccination Status, and Emerging Oral Antivirals.Thromb Haemost. 2023 Feb;123(2):186-191. doi: 10.1055/a-1956-9641. Epub 2022 Oct 7. Thromb Haemost. 2023. PMID: 36206775 Free PMC article.
-
Platelet and Endothelial Activation as Potential Mechanisms Behind the Thrombotic Complications of COVID-19 Patients.JACC Basic Transl Sci. 2021 Mar;6(3):202-218. doi: 10.1016/j.jacbts.2020.12.009. Epub 2021 Feb 24. JACC Basic Transl Sci. 2021. PMID: 33649738 Free PMC article.
References
-
- World Health Organization Coronavirus Disease 2019 (COVID-19) Situation report - 46. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2... Available at: Accessed on March 12 2020.
-
- Clerkin K.J., Fried J.A., Rakhelkar J. Coronavirus disease 2019 (COVID-19) and cardiovascular disease. Circulation. 2020 Mar 21 [E-pub ahead of print]
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
