

A soluble phosphorylated tau signature links tau, amyloid and the evolution of stages of dominantly inherited Alzheimer's disease
- PMID: 32161412
- PMCID: PMC7309367
- DOI: 10.1038/s41591-020-0781-z
A soluble phosphorylated tau signature links tau, amyloid and the evolution of stages of dominantly inherited Alzheimer's disease
Abstract
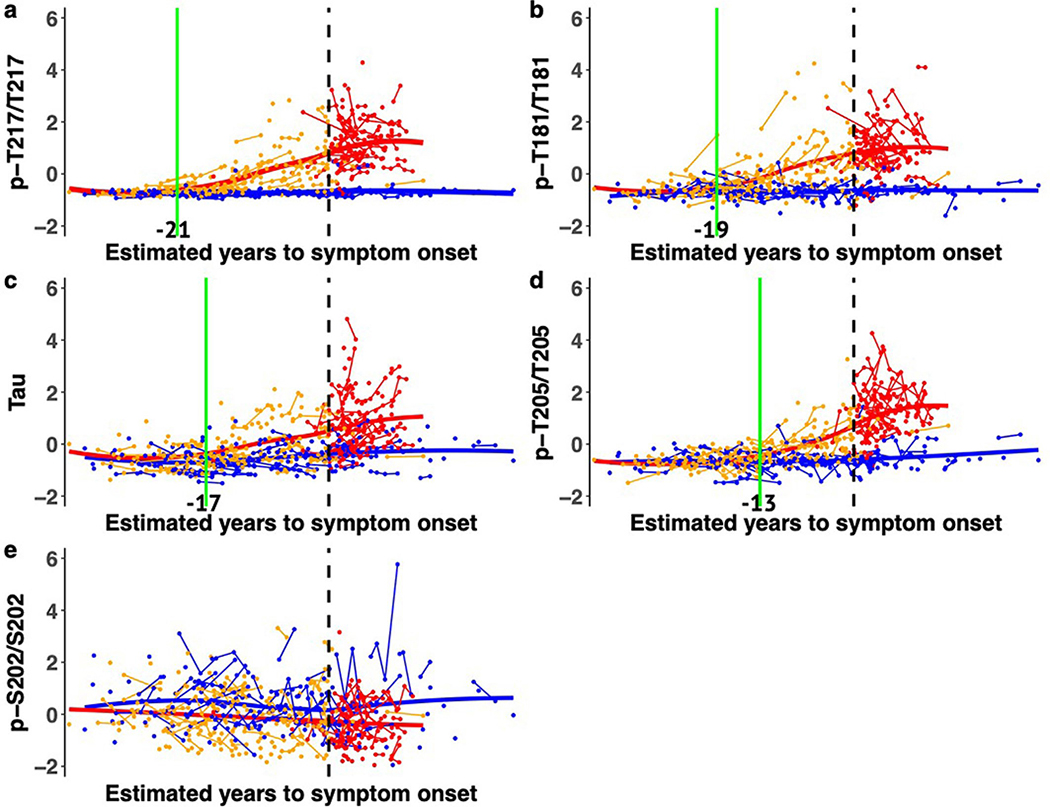
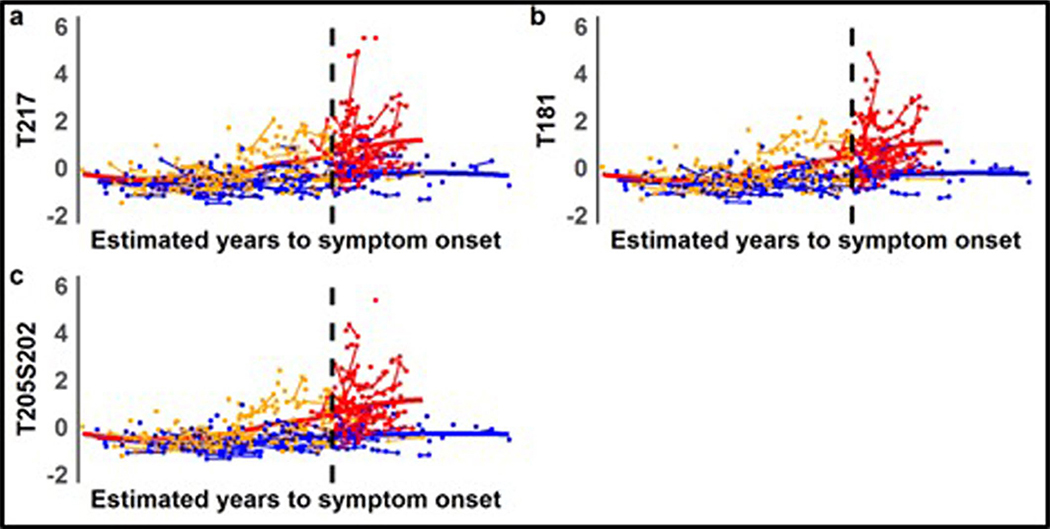
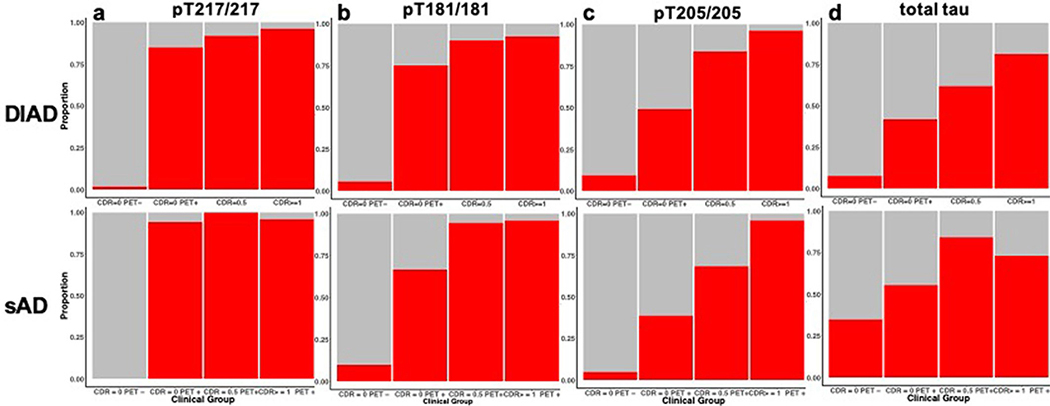
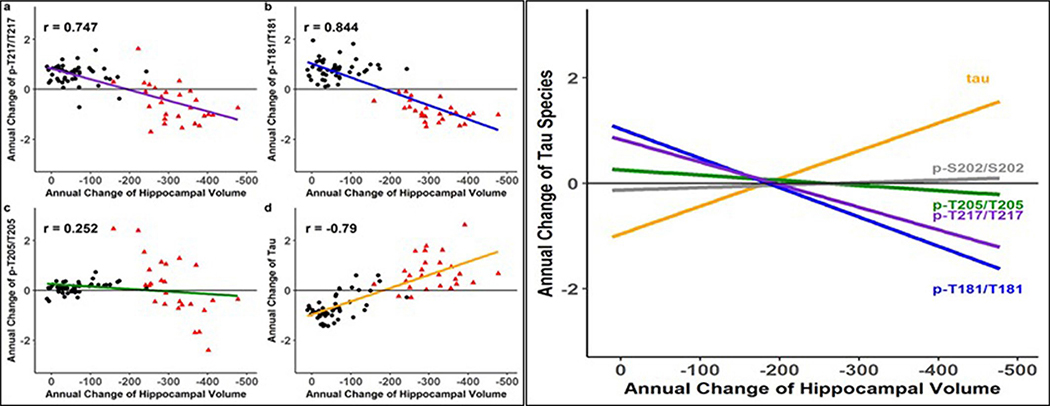
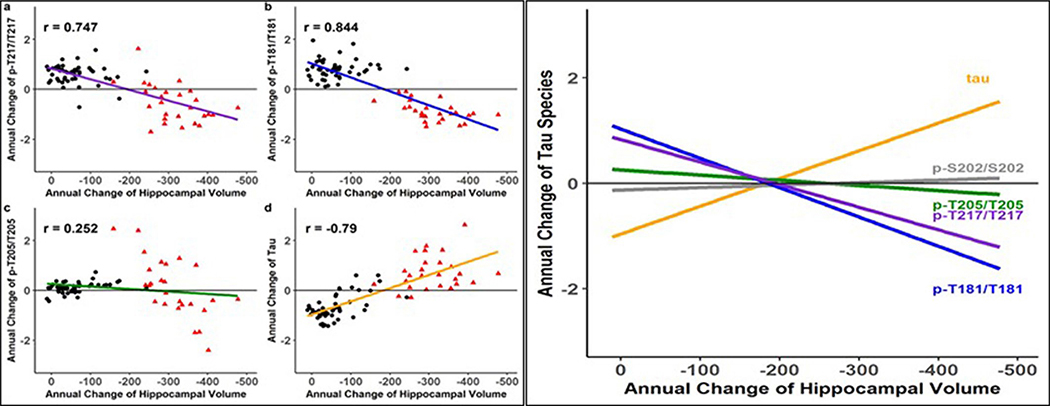
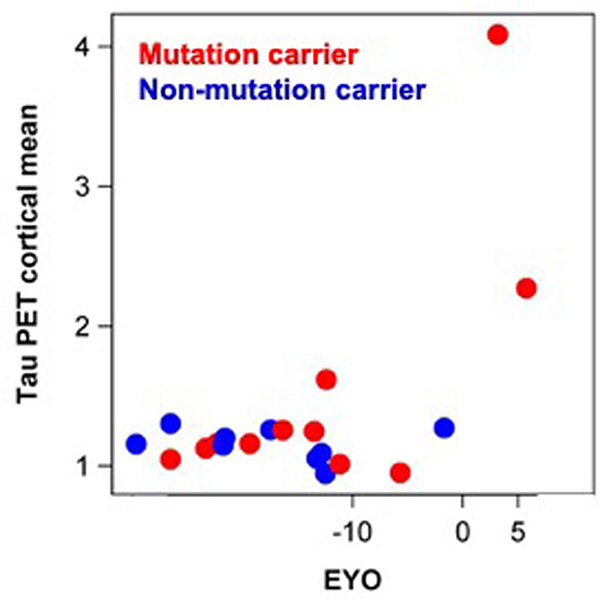
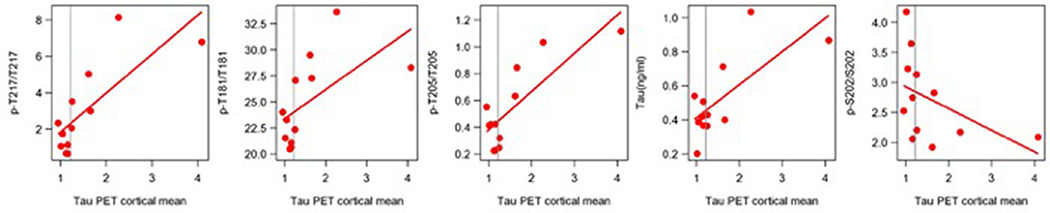
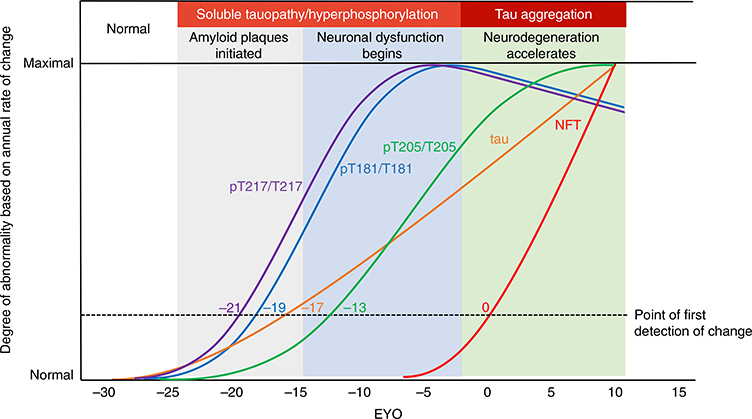
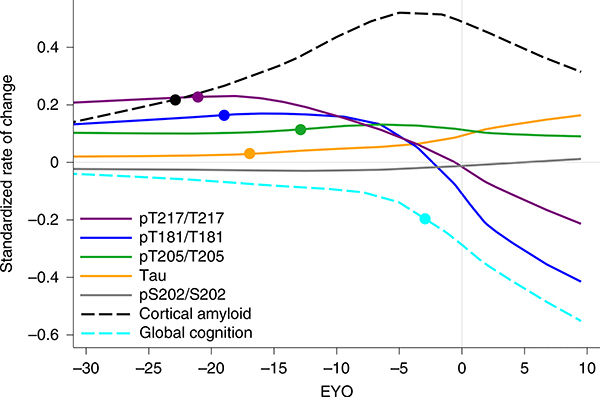
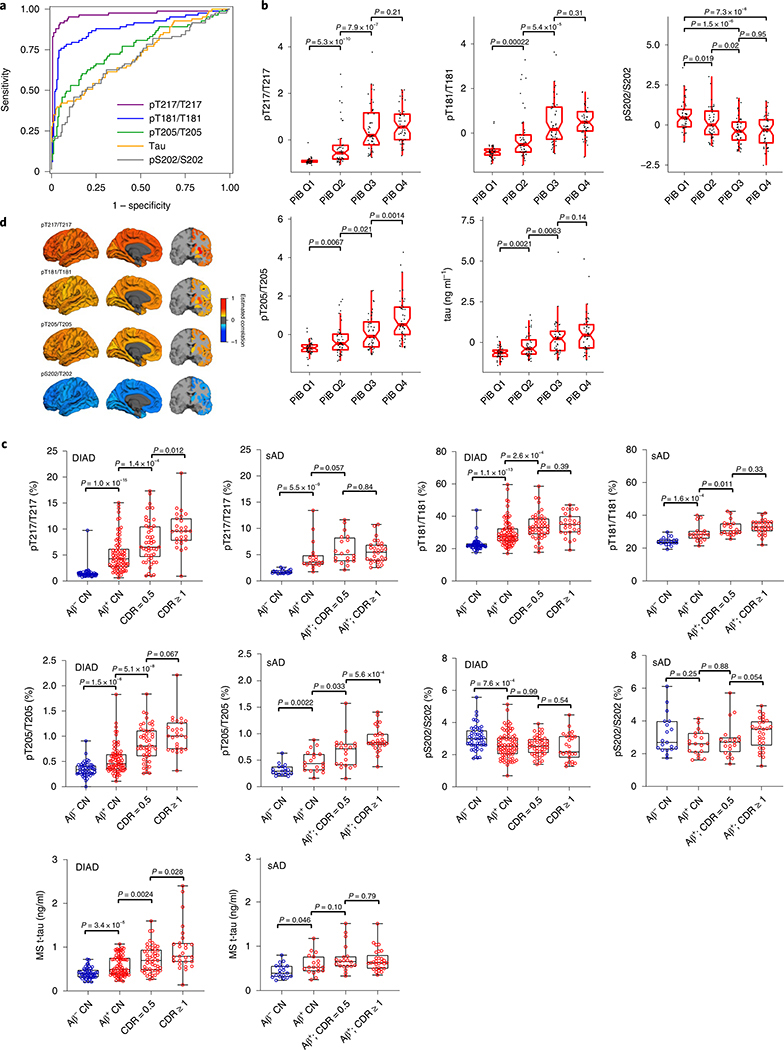
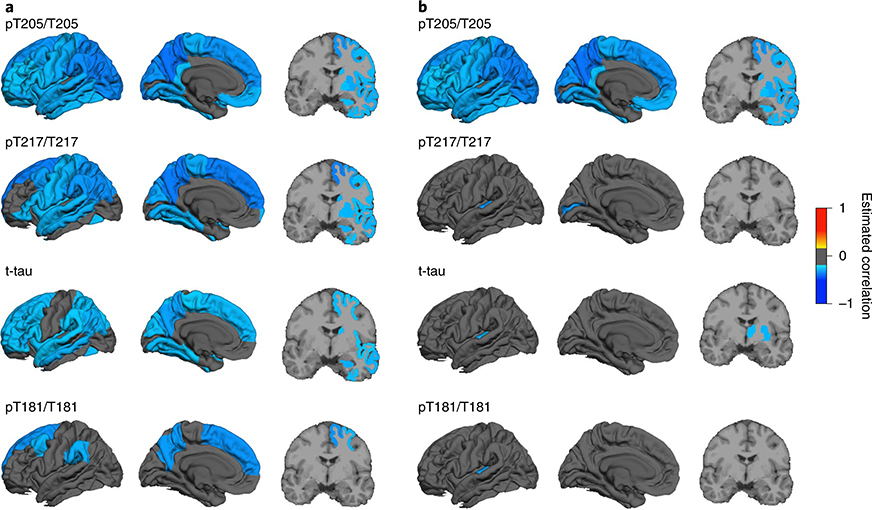
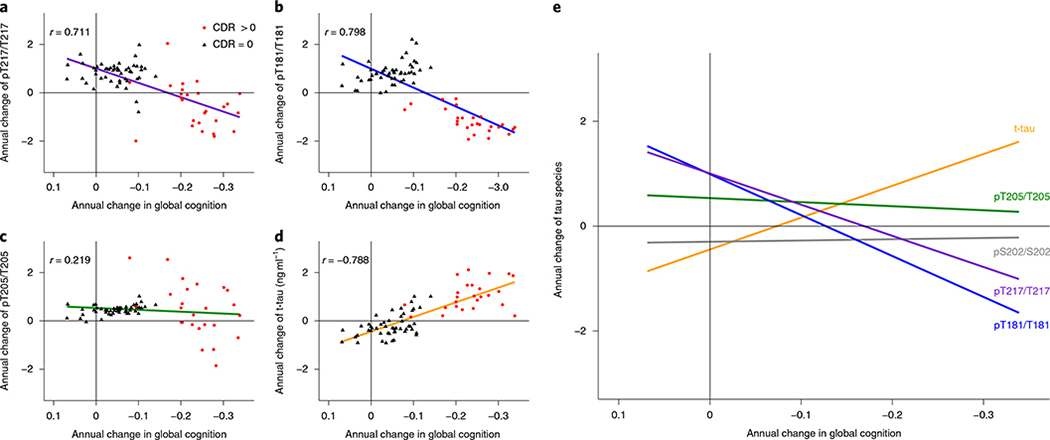
Development of tau-based therapies for Alzheimer's disease requires an understanding of the timing of disease-related changes in tau. We quantified the phosphorylation state at multiple sites of the tau protein in cerebrospinal fluid markers across four decades of disease progression in dominantly inherited Alzheimer's disease. We identified a pattern of tau staging where site-specific phosphorylation changes occur at different periods of disease progression and follow distinct trajectories over time. These tau phosphorylation state changes are uniquely associated with structural, metabolic, neurodegenerative and clinical markers of disease, and some (p-tau217 and p-tau181) begin with the initial increases in aggregate amyloid-β as early as two decades before the development of aggregated tau pathology. Others (p-tau205 and t-tau) increase with atrophy and hypometabolism closer to symptom onset. These findings provide insights into the pathways linking tau, amyloid-β and neurodegeneration, and may facilitate clinical trials of tau-based treatments.
Conflict of interest statement
Competing interests
R.J.B. has equity ownership interest in C2N Diagnostics and receives royalty income based on technology (stable isotope labeling kinetics and blood plasma assay) licensed by Washington University to C2N Diagnostics. R.J.B. receives income from C2N Diagnostics for serving on the scientific advisory board. Washington University, with R.J.B., E.M. and N.R.B. as co-inventors, has submitted the US nonprovisional patent application ‘Cerebrospinal fluid (CSF) tau rate of phosphorylation measurement to define stages of Alzheimer’s disease and monitor brain kinases/phosphatases activity’. R.J.B. has received honoraria from Janssen and Pfizer as a speaker, and from Merck and Pfizer as an advisory board member. E.M. has received royalty payments for an educational program supported by Eli Lilly and as a member of a scientific advisory board for Eli Lilly.
Figures

Similar articles
-
Association of BDNF Val66Met With Tau Hyperphosphorylation and Cognition in Dominantly Inherited Alzheimer Disease.JAMA Neurol. 2022 Mar 1;79(3):261-270. doi: 10.1001/jamaneurol.2021.5181. JAMA Neurol. 2022. PMID: 35099506 Free PMC article.
-
Comparison of Plasma Phosphorylated Tau Species With Amyloid and Tau Positron Emission Tomography, Neurodegeneration, Vascular Pathology, and Cognitive Outcomes.JAMA Neurol. 2021 Sep 1;78(9):1108-1117. doi: 10.1001/jamaneurol.2021.2293. JAMA Neurol. 2021. PMID: 34309632 Free PMC article.
-
Association of Longitudinal Changes in Cerebrospinal Fluid Total Tau and Phosphorylated Tau 181 and Brain Atrophy With Disease Progression in Patients With Alzheimer Disease.JAMA Netw Open. 2019 Dec 2;2(12):e1917126. doi: 10.1001/jamanetworkopen.2019.17126. JAMA Netw Open. 2019. PMID: 31825500 Free PMC article.
-
Tau biomarkers in Alzheimer's disease: towards implementation in clinical practice and trials.Lancet Neurol. 2022 Aug;21(8):726-734. doi: 10.1016/S1474-4422(22)00168-5. Epub 2022 May 25. Lancet Neurol. 2022. PMID: 35643092 Review.
-
Understanding disease progression and improving Alzheimer's disease clinical trials: Recent highlights from the Alzheimer's Disease Neuroimaging Initiative.Alzheimers Dement. 2019 Jan;15(1):106-152. doi: 10.1016/j.jalz.2018.08.005. Epub 2018 Oct 13. Alzheimers Dement. 2019. PMID: 30321505 Review.
Cited by
-
Modeling the temporal evolution of plasma p-tau in relation to amyloid beta and tau PET.Alzheimers Dement. 2024 Feb;20(2):1225-1238. doi: 10.1002/alz.13539. Epub 2023 Nov 14. Alzheimers Dement. 2024. PMID: 37963289 Free PMC article.
-
Protein Biomarkers for the Diagnosis of Alzheimer's Disease at Different Stages of Neurodegeneration.Int J Mol Sci. 2020 Sep 15;21(18):6749. doi: 10.3390/ijms21186749. Int J Mol Sci. 2020. PMID: 32942527 Free PMC article. Review.
-
Developmental neurotoxicity of PFOA exposure on hiPSC-derived cortical neurons.Environ Int. 2024 Aug;190:108914. doi: 10.1016/j.envint.2024.108914. Epub 2024 Jul 26. Environ Int. 2024. PMID: 39079332 Free PMC article.
-
Soluble P-tau217 reflects amyloid and tau pathology and mediates the association of amyloid with tau.EMBO Mol Med. 2021 Jun 7;13(6):e14022. doi: 10.15252/emmm.202114022. Epub 2021 May 5. EMBO Mol Med. 2021. PMID: 33949133 Free PMC article.
-
Targeting tau in Alzheimer's disease: from mechanisms to clinical therapy.Neural Regen Res. 2024 Jul 1;19(7):1489-1498. doi: 10.4103/1673-5374.385847. Epub 2023 Sep 22. Neural Regen Res. 2024. PMID: 38051891 Free PMC article.
References
-
- Goedert M, Spillantini MG, Jakes R, Rutherford D & Crowther RA Multiple isoforms of human microtubule-associated protein tau: sequences and localization in neurofibrillary tangles of Alzheimer’s disease. Neuron 3, 519–526 (1989). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AG066444/AG/NIA NIH HHS/United States
- R01NS095773/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)/International
- K23 AG046363/AG/NIA NIH HHS/United States
- UF1 AG032438/AG/NIA NIH HHS/United States
- U19 AG032438/AG/NIA NIH HHS/United States
- UF1AG032438/U.S. Department of Health & Human Services | NIH | National Institute on Aging (U.S. National Institute on Aging)/International
- MR/L023784/1/RCUK | Medical Research Council (MRC)/International
- MR/009076/1/RCUK | Medical Research Council (MRC)/International
- P50 AG005681/AG/NIA NIH HHS/United States
- MR/L023784/1/U.S. Department of Health & Human Services | NIH | National Institute on Aging (U.S. National Institute on Aging)/International
- R01 AG052550/AG/NIA NIH HHS/United States
- R01 NS095773/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
