

The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017
- PMID: 31981519
- PMCID: PMC7026710
- DOI: 10.1016/S2468-1253(19)30349-8
The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017
Abstract
Background: Cirrhosis and other chronic liver diseases (collectively referred to as cirrhosis in this paper) are a major cause of morbidity and mortality globally, although the burden and underlying causes differ across locations and demographic groups. We report on results from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2017 on the burden of cirrhosis and its trends since 1990, by cause, sex, and age, for 195 countries and territories.
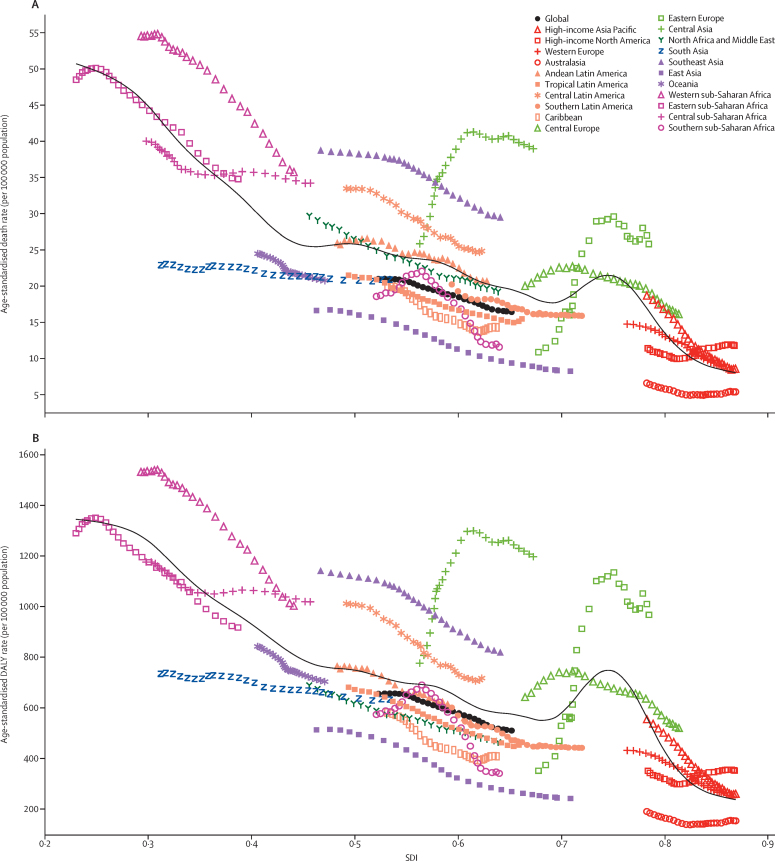
Methods: We used data from vital registrations, vital registration samples, and verbal autopsies to estimate mortality. We modelled prevalence of total, compensated, and decompensated cirrhosis on the basis of hospital and claims data. Disability-adjusted life-years (DALYs) were calculated as the sum of years of life lost due to premature death and years lived with disability. Estimates are presented as numbers and age-standardised or age-specific rates per 100 000 population, with 95% uncertainty intervals (UIs). All estimates are presented for five causes of cirrhosis: hepatitis B, hepatitis C, alcohol-related liver disease, non-alcoholic steatohepatitis (NASH), and other causes. We compared mortality, prevalence, and DALY estimates with those expected according to the Socio-demographic Index (SDI) as a proxy for the development status of regions and countries.
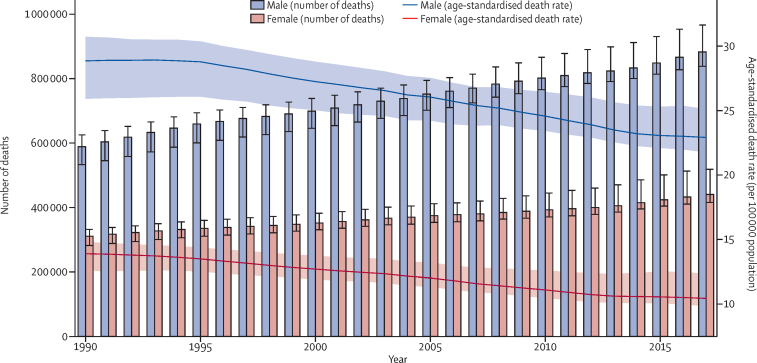
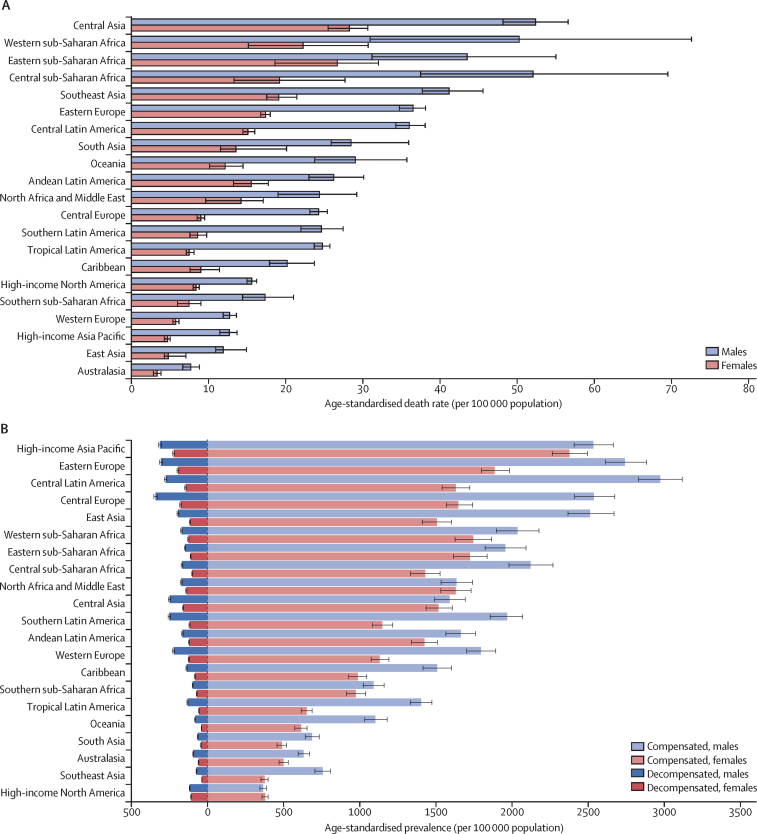
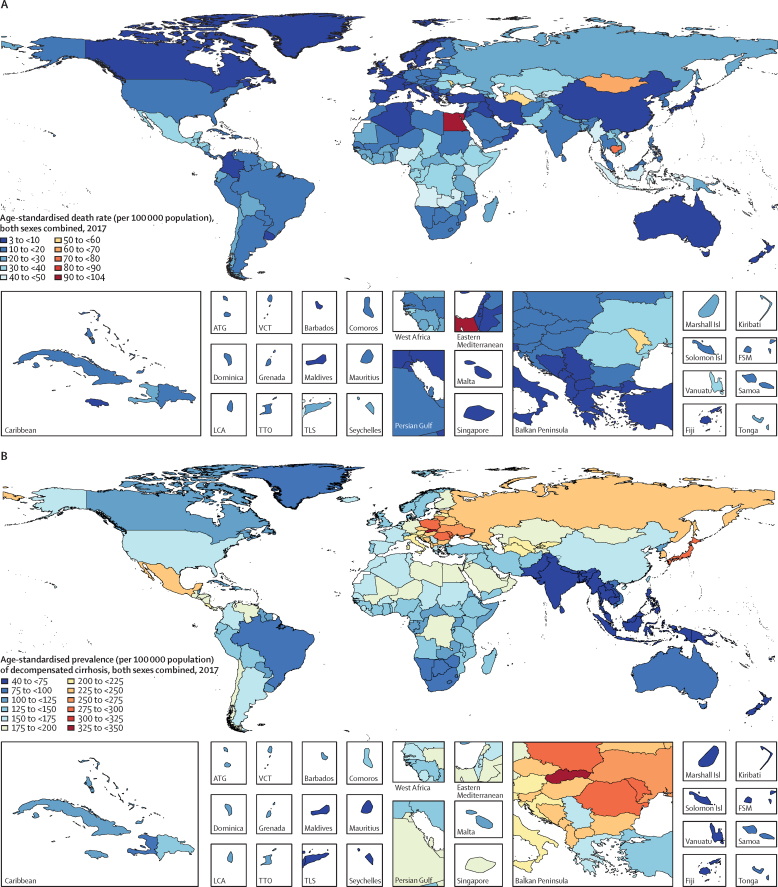
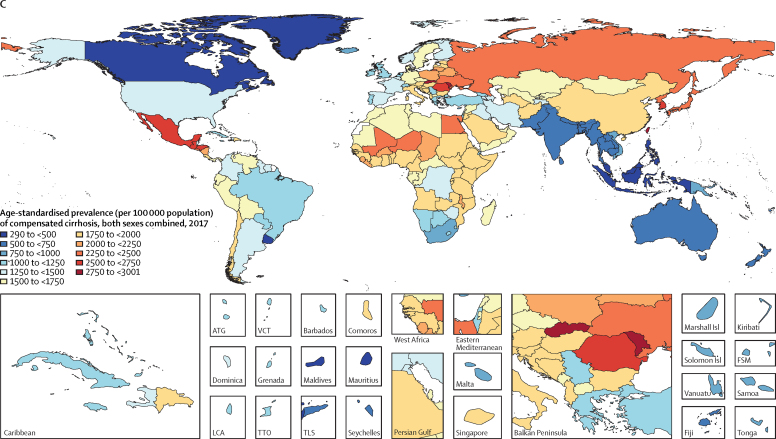
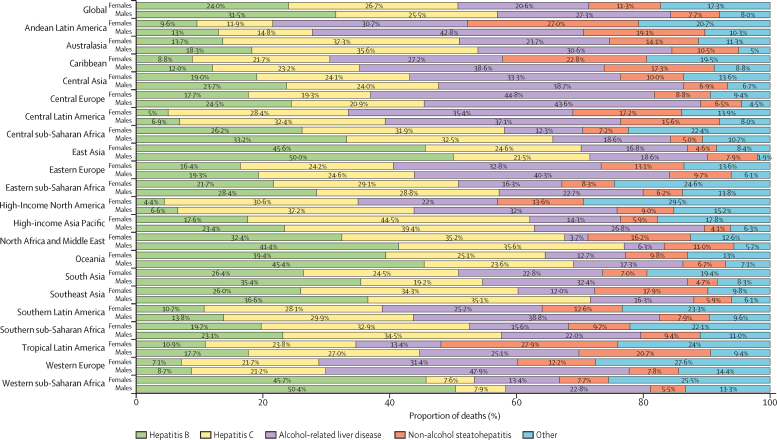
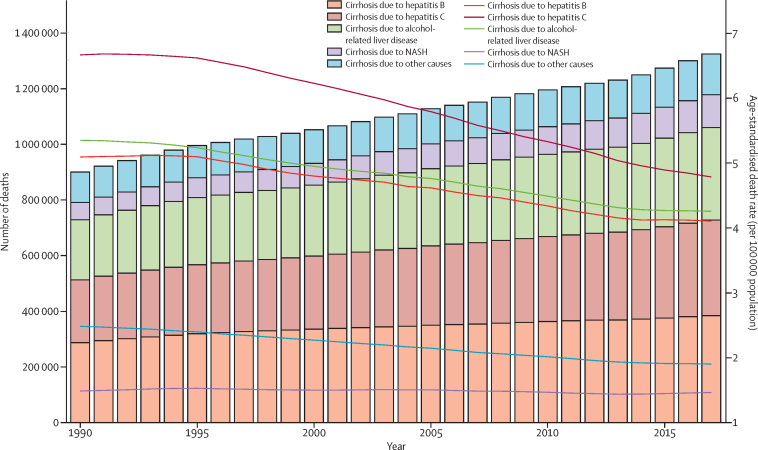
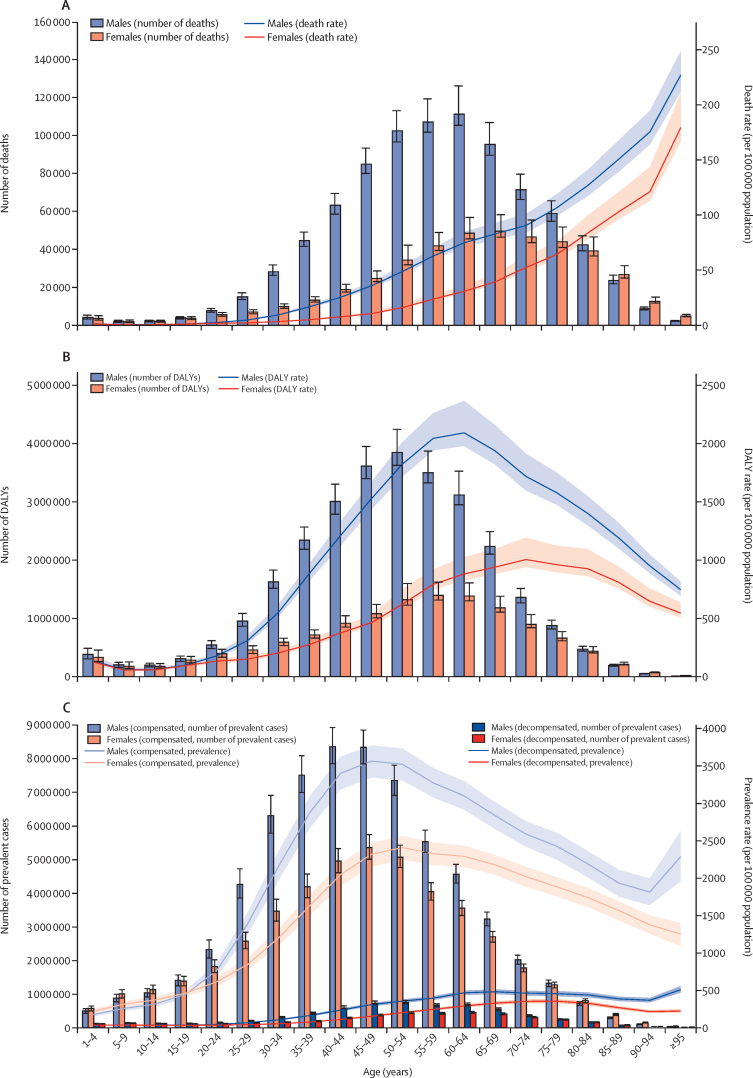
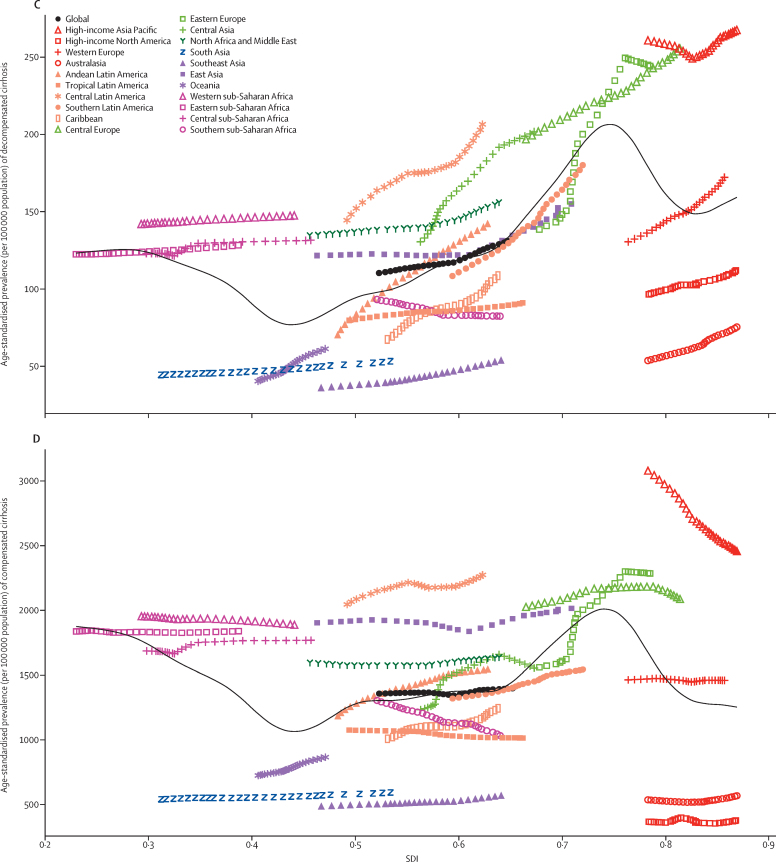
Findings: In 2017, cirrhosis caused more than 1·32 million (95% UI 1·27-1·45) deaths (440 000 [416 000-518 000; 33·3%] in females and 883 000 [838 000-967 000; 66·7%] in males) globally, compared with less than 899 000 (829 000-948 000) deaths in 1990. Deaths due to cirrhosis constituted 2·4% (2·3-2·6) of total deaths globally in 2017 compared with 1·9% (1·8-2·0) in 1990. Despite an increase in the number of deaths, the age-standardised death rate decreased from 21·0 (19·2-22·3) per 100 000 population in 1990 to 16·5 (15·8-18·1) per 100 000 population in 2017. Sub-Saharan Africa had the highest age-standardised death rate among GBD super-regions for all years of the study period (32·2 [25·8-38·6] deaths per 100 000 population in 2017), and the high-income super-region had the lowest (10·1 [9·8-10·5] deaths per 100 000 population in 2017). The age-standardised death rate decreased or remained constant from 1990 to 2017 in all GBD regions except eastern Europe and central Asia, where the age-standardised death rate increased, primarily due to increases in alcohol-related liver disease prevalence. At the national level, the age-standardised death rate of cirrhosis was lowest in Singapore in 2017 (3·7 [3·3-4·0] per 100 000 in 2017) and highest in Egypt in all years since 1990 (103·3 [64·4-133·4] per 100 000 in 2017). There were 10·6 million (10·3-10·9) prevalent cases of decompensated cirrhosis and 112 million (107-119) prevalent cases of compensated cirrhosis globally in 2017. There was a significant increase in age-standardised prevalence rate of decompensated cirrhosis between 1990 and 2017. Cirrhosis caused by NASH had a steady age-standardised death rate throughout the study period, whereas the other four causes showed declines in age-standardised death rate. The age-standardised prevalence of compensated and decompensated cirrhosis due to NASH increased more than for any other cause of cirrhosis (by 33·2% for compensated cirrhosis and 54·8% for decompensated cirrhosis) over the study period. From 1990 to 2017, the number of prevalent cases more than doubled for compensated cirrhosis due to NASH and more than tripled for decompensated cirrhosis due to NASH. In 2017, age-standardised death and DALY rates were lower among countries and territories with higher SDI.
Interpretation: Cirrhosis imposes a substantial health burden on many countries and this burden has increased at the global level since 1990, partly due to population growth and ageing. Although the age-standardised death and DALY rates of cirrhosis decreased from 1990 to 2017, numbers of deaths and DALYs and the proportion of all global deaths due to cirrhosis increased. Despite the availability of effective interventions for the prevention and treatment of hepatitis B and C, they were still the main causes of cirrhosis burden worldwide, particularly in low-income countries. The impact of hepatitis B and C is expected to be attenuated and overtaken by that of NASH in the near future. Cost-effective interventions are required to continue the prevention and treatment of viral hepatitis, and to achieve early diagnosis and prevention of cirrhosis due to alcohol-related liver disease and NASH.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Similar articles
-
Burden of disease scenarios for 204 countries and territories, 2022-2050: a forecasting analysis for the Global Burden of Disease Study 2021.Lancet. 2024 May 18;403(10440):2204-2256. doi: 10.1016/S0140-6736(24)00685-8. Lancet. 2024. PMID: 38762325 Free PMC article.
-
Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017.Lancet. 2018 Nov 10;392(10159):1923-1994. doi: 10.1016/S0140-6736(18)32225-6. Epub 2018 Nov 8. Lancet. 2018. PMID: 30496105 Free PMC article.
-
Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016.Lancet. 2017 Sep 16;390(10100):1151-1210. doi: 10.1016/S0140-6736(17)32152-9. Lancet. 2017. PMID: 28919116 Free PMC article.
-
Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.Lancet. 2015 Aug 22;386(9995):743-800. doi: 10.1016/S0140-6736(15)60692-4. Epub 2015 Jun 7. Lancet. 2015. PMID: 26063472 Free PMC article. Review.
-
Alcohol use and burden for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016.Lancet. 2018 Sep 22;392(10152):1015-1035. doi: 10.1016/S0140-6736(18)31310-2. Epub 2018 Aug 23. Lancet. 2018. PMID: 30146330 Free PMC article. Review.
Cited by
-
Multiparametric MR mapping in clinical decision-making for diffuse liver disease.Abdom Radiol (NY). 2020 Nov;45(11):3507-3522. doi: 10.1007/s00261-020-02684-3. Epub 2020 Aug 5. Abdom Radiol (NY). 2020. PMID: 32761254 Free PMC article. Review.
-
Muscle-Invasive Bladder Cancer in Patients with Liver Cirrhosis: A Review of Pertinent Considerations.Bladder Cancer. 2021 Aug 31;7(3):261-278. doi: 10.3233/BLC-211536. eCollection 2021. Bladder Cancer. 2021. PMID: 38993608 Free PMC article. Review.
-
Endoscopic Band Ligation Versus Argon Plasma Coagulation in the Treatment of Gastric Antral Vascular Ectasia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Clin Endosc. 2021 Sep;54(5):669-677. doi: 10.5946/ce.2021.063. Epub 2021 May 31. Clin Endosc. 2021. PMID: 34053215 Free PMC article.
-
Disease burden of chronic hepatitis B and complications in China from 2006 to 2050: an individual-based modeling study.Virol J. 2020 Aug 28;17(1):132. doi: 10.1186/s12985-020-01393-z. Virol J. 2020. PMID: 32859216 Free PMC article.
-
Worldwide long-term trends in the incidence of nonalcoholic fatty liver disease during 1990-2019: A joinpoint and age-period-cohort analysis.Front Cardiovasc Med. 2022 Sep 12;9:891963. doi: 10.3389/fcvm.2022.891963. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36172576 Free PMC article.
References
-
- Fleming KM, Aithal GP, Card TR, West J. The rate of decompensation and clinical progression of disease in people with cirrhosis: a cohort study. Aliment Pharmacol Ther. 2010;32:1343–1350. - PubMed
-
- Moreau R, Jalan R, Gines P. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013;144:1426. 37.e1-9. - PubMed
-
- D'Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44:217–231. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
