

Impact of intensive care unit supportive care on the physiology of Ebola virus disease in a universally lethal non-human primate model
- PMID: 31520194
- PMCID: PMC6744539
- DOI: 10.1186/s40635-019-0268-8
Impact of intensive care unit supportive care on the physiology of Ebola virus disease in a universally lethal non-human primate model
Erratum in
-
Correction to: Impact of intensive care unit supportive care on the physiology of Ebola virus disease in a universally lethal non-human primate model.Intensive Care Med Exp. 2019 Dec 4;7(1):66. doi: 10.1186/s40635-019-0283-9. Intensive Care Med Exp. 2019. PMID: 31802320 Free PMC article.
Abstract
Background: There are currently limited data for the use of specific antiviral therapies for the treatment of Ebola virus disease (EVD). While there is anecdotal evidence that supportive care may be effective, there is a paucity of direct experimental data to demonstrate a role for supportive care in EVD. We studied the impact of ICU-level supportive care interventions including fluid resuscitation, vasoactive medications, blood transfusion, hydrocortisone, and ventilator support on the pathophysiology of EVD in rhesus macaques infected with a universally lethal dose of Ebola virus strain Makona C07.
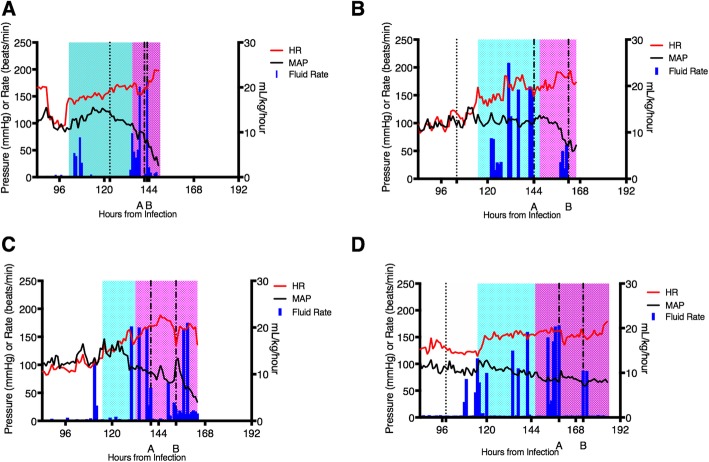
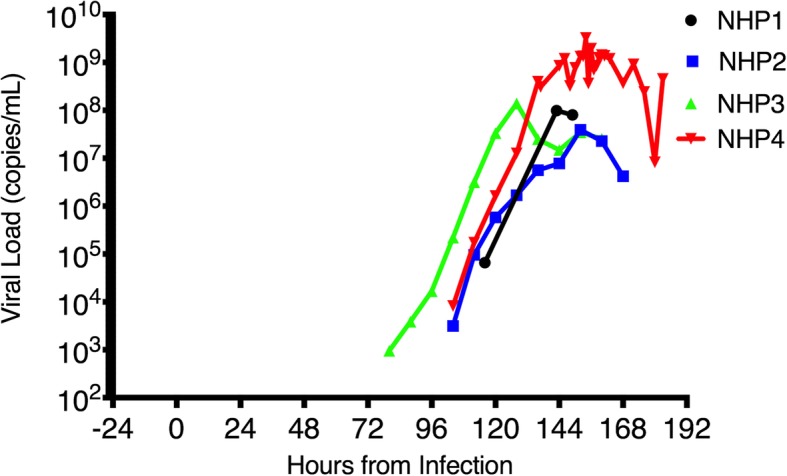
Methods: Four NHPs were infected with a universally lethal dose Ebola virus strain Makona, in accordance with the gold standard lethal Ebola NHP challenge model. Following infection, the following therapeutic interventions were employed: continuous bedside supportive care, ventilator support, judicious fluid resuscitation, vasoactive medications, blood transfusion, and hydrocortisone as needed to treat cardiovascular compromise. A range of physiological parameters were continuously monitored to gage any response to the interventions.
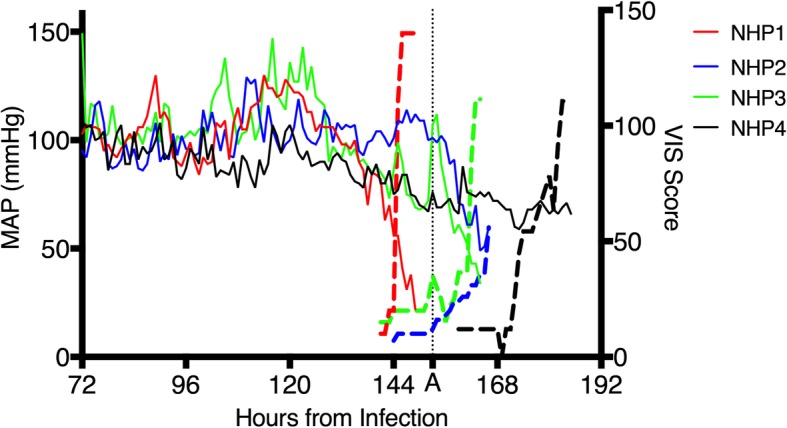
Results: All four NHPs developed EVD and demonstrated a similar clinical course. All animals reached a terminal endpoint, which occurred at an average time of 166.5 ± 14.8 h post-infection. Fluid administration may have temporarily blunted a rise in lactate, but the effect was short lived. Vasoactive medications resulted in short-lived improvements in mean arterial pressure. Blood transfusion and hydrocortisone did not appear to have a significant positive impact on the course of the disease.
Conclusions: The model employed for this study is reflective of an intramuscular infection in humans (e.g., needle stick) and is highly lethal to NHPs. Using this model, we found that the animals developed progressive severe organ dysfunction and profound shock preceding death. While the overall impact of supportive care on the observed pathophysiology was limited, we did observe some time-dependent positive responses. Since this model is highly lethal, it does not reflect the full spectrum of human EVD. Our findings support the need for continued development of animal models that replicate the spectrum of human disease as well as ongoing development of anti-Ebola therapies to complement supportive care.
Keywords: Ebola; Fluid; Hydrocortisone; NHP; Pathophysiology; Supportive care; Vasoactives; Ventilatory support.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Intensive Care Unit-Like Care of Nonhuman Primates with Ebola Virus Disease.J Infect Dis. 2021 Aug 16;224(4):632-642. doi: 10.1093/infdis/jiaa781. J Infect Dis. 2021. PMID: 33367826 Free PMC article.
-
Antiviral efficacy of favipiravir against Ebola virus: A translational study in cynomolgus macaques.PLoS Med. 2018 Mar 27;15(3):e1002535. doi: 10.1371/journal.pmed.1002535. eCollection 2018 Mar. PLoS Med. 2018. PMID: 29584730 Free PMC article.
-
Clinical Laboratory Values as Early Indicators of Ebola Virus Infection in Nonhuman Primates.Emerg Infect Dis. 2017 Aug;23(8):1316-1324. doi: 10.3201/eid2308.170029. Emerg Infect Dis. 2017. PMID: 28726603 Free PMC article.
-
Clinical presentation and management of severe Ebola virus disease.Ann Am Thorac Soc. 2014 Nov;11(9):1341-50. doi: 10.1513/AnnalsATS.201410-481PS. Ann Am Thorac Soc. 2014. PMID: 25369317 Review.
-
Treatment of ebola virus disease.Pharmacotherapy. 2015 Jan;35(1):43-53. doi: 10.1002/phar.1545. Pharmacotherapy. 2015. PMID: 25630412 Review.
Cited by
-
Clinical and Immunologic Correlates of Vasodilatory Shock Among Ebola Virus-Infected Nonhuman Primates in a Critical Care Model.J Infect Dis. 2023 Nov 13;228(Suppl 7):S635-S647. doi: 10.1093/infdis/jiad374. J Infect Dis. 2023. PMID: 37652048 Free PMC article.
-
Characterization of Ebola Virus Risk to Bedside Providers in an Intensive Care Environment.Microorganisms. 2021 Feb 26;9(3):498. doi: 10.3390/microorganisms9030498. Microorganisms. 2021. PMID: 33652895 Free PMC article.
-
The Emergence of Travel-related Infections in Critical Care Units.J Transl Int Med. 2022 Nov 23;10(4):328-339. doi: 10.2478/jtim-2022-0042. eCollection 2022 Dec. J Transl Int Med. 2022. PMID: 36860632 Free PMC article.
-
Immunotherapeutics for Ebola Virus Disease: Hope on the Horizon.Biologics. 2021 Mar 18;15:79-86. doi: 10.2147/BTT.S259069. eCollection 2021. Biologics. 2021. PMID: 33776420 Free PMC article. Review.
-
Correction to: Impact of intensive care unit supportive care on the physiology of Ebola virus disease in a universally lethal non-human primate model.Intensive Care Med Exp. 2019 Dec 4;7(1):66. doi: 10.1186/s40635-019-0283-9. Intensive Care Med Exp. 2019. PMID: 31802320 Free PMC article.
References
-
- WHO . Ebola situation reports: Democratic Republic of the Congo. Geneva: Ebola situation reports: Democratic Republic of the Congo; 2018.
-
- Fowler RA, Fletcher T, Fischer WA, 2nd, Lamontagne F, Jacob S, Brett-Major D, Lawler JV, Jacquerioz FA, Houlihan C, O'Dempsey T, Ferri M, Adachi T, Lamah MC, Bah EI, Mayet T, Schieffelin J, McLellan SL, Senga M, Kato Y, Clement C, Mardel S, Vallenas Bejar De Villar RC, Shindo N, Bausch D. Caring for critically ill patients with ebola virus disease. Perspectives from West Africa. Am J Respir Crit Care Med. 2014;190:733–737. doi: 10.1164/rccm.201408-1514CP. - DOI - PubMed
-
- Guimard Y, Bwaka MA, Colebunders R, Calain P, Massaba M, De Roo A, Mupapa KD, Kibadi K, Kuvula KJ, Ndaberey E, Katwiki KR, Mapanda BB, Nkuku OB, Fleerackers Y, Van den Enden E, Kipasa MA. Organization of patient care during the Ebola hemorrhagic fever epidemic in Kikwit, Democratic Republic of Congo, 1995. J Infect Dis. 1999;179:S268–S273. doi: 10.1086/514315. - DOI - PubMed
-
- Lamontagne F, Fowler RA, Adhikari NK, Murthy S, Brett-Major DM, Jacobs M, Uyeki TM, Vallenas C, Norris SL, Fischer WA, Fletcher TE, Levine AC, Reed P, Bausch DG, Gove S, Hall A, Shepherd S, Siemieniuk RA, Lamah M-C, Kamara R, Nakyeyune P, Soka MJ, Edwin A, Hazzan AA, Jacob ST, Elkarsany MM, Adachi T, Benhadj L, Clément C, Crozier I, Garcia A, Hoffman SJ, Guyatt GH (2017) Evidence-based guidelines for supportive care of patients with Ebola virus disease. Lancet - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
