

A multicenter RCT of noninvasive ventilation in pneumonia-induced early mild acute respiratory distress syndrome
- PMID: 31484582
- PMCID: PMC6727327
- DOI: 10.1186/s13054-019-2575-6
A multicenter RCT of noninvasive ventilation in pneumonia-induced early mild acute respiratory distress syndrome
Abstract
Rationale: Our pilot study suggested that noninvasive ventilation (NIV) reduced the need for intubation compared with conventional administration of oxygen on patients with "early" stage of mild acute respiratory distress syndrome (ARDS, PaO2/FIO2 between 200 and 300).
Objectives: To evaluate whether early NIV can reduce the need for invasive ventilation in patients with pneumonia-induced early mild ARDS.
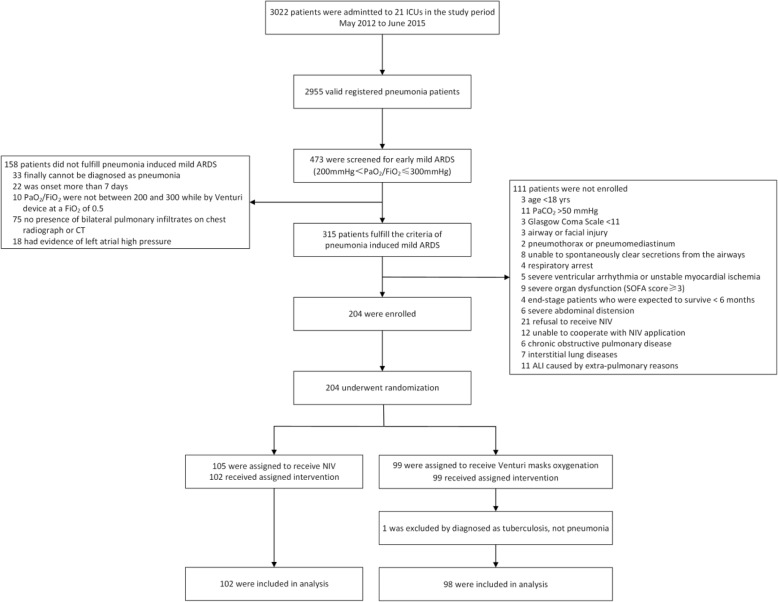
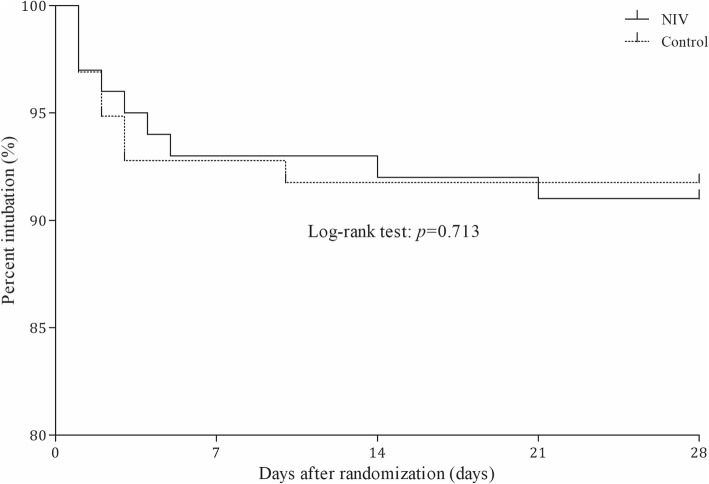
Methods: Prospective, multicenter, randomized controlled trial (RCT) of NIV compared with conventional administration of oxygen through a Venturi mask. Primary outcome included the numbers of patients who met the intubation criteria.
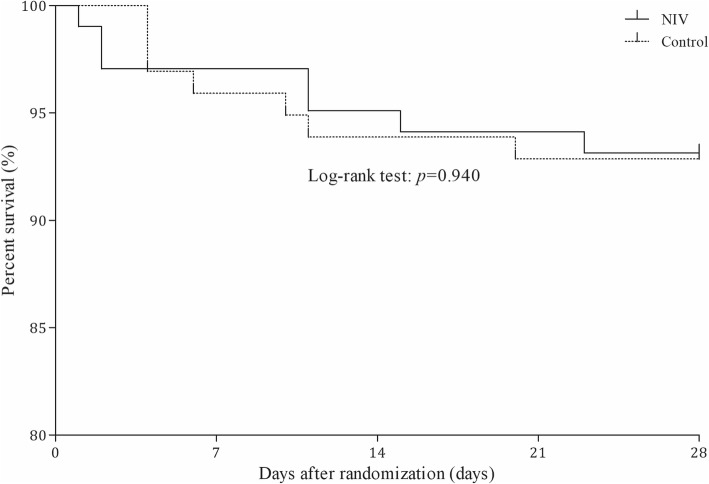
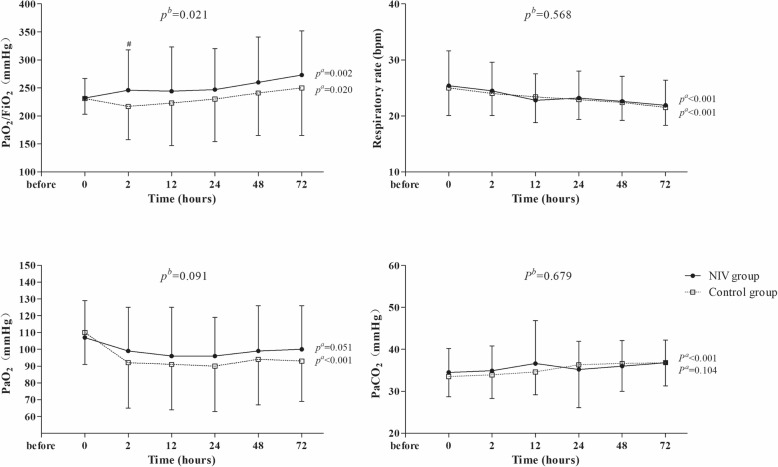
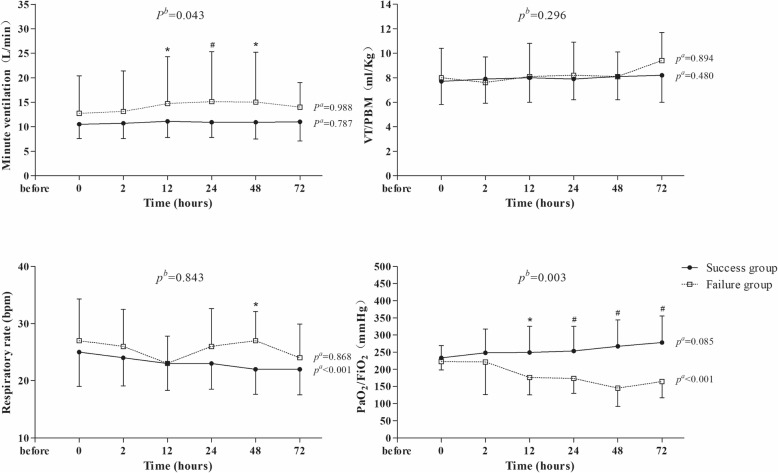
Results: Two hundred subjects were randomized to NIV (n = 102) or control (n = 98) groups from 21 centers. Baseline characteristics were similar in the two groups. In the NIV group, PaO2/FIO2 became significantly higher than in the control group at 2 h after randomization and remained stable for the first 72 h. NIV did not decrease the proportion of patients requiring intubation than in the control group (11/102 vs. 9/98, 10.8% vs. 9.2%, p = 0.706). The ICU mortality was similar in the two groups (7/102 vs. 7/98, 4.9% vs. 3.1%, p = 0.721). Multivariate analysis showed minute ventilation greater than 11 L/min at 48 h was the independent risk factor for NIV failure (OR, 1.176 [95% CI, 1.005-1.379], p = 0.043).
Conclusions: Treatment with NIV did not reduce the need for intubation among patients with pneumonia-induced early mild ARDS, despite the improved PaO2/FIO2 observed with NIV compared with standard oxygen therapy. High minute ventilation may predict NIV failure.
Trial registration: NCT01581229 . Registered 19 April 2012.
Keywords: Acute respiratory distress syndrome (ARDS); Noninvasive ventilation (NIV); Pneumonia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Noninvasive ventilation in patients with acute respiratory distress syndrome.Crit Care. 2019 Nov 15;23(1):358. doi: 10.1186/s13054-019-2666-4. Crit Care. 2019. PMID: 31730002 Free PMC article. No abstract available.
Similar articles
-
[Study of timing of invasive and noninvasive sequential ventilation in patients with acute respiratory distress syndrome].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014 May;26(5):330-4. doi: 10.3760/cma.j.issn.2095-4352.2014.05.009. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014. PMID: 24809262 Clinical Trial. Chinese.
-
Sequential application of oxygen therapy via high-flow nasal cannula and noninvasive ventilation in acute respiratory failure: an observational pilot study.Respir Care. 2015 Feb;60(2):170-8. doi: 10.4187/respcare.03075. Epub 2014 Oct 7. Respir Care. 2015. PMID: 25294935
-
Noninvasive Ventilation of Patients with Acute Respiratory Distress Syndrome. Insights from the LUNG SAFE Study.Am J Respir Crit Care Med. 2017 Jan 1;195(1):67-77. doi: 10.1164/rccm.201606-1306OC. Am J Respir Crit Care Med. 2017. PMID: 27753501
-
Safety and efficacy of noninvasive ventilation in patients with blunt chest trauma: a systematic review.Crit Care. 2013 Jul 22;17(4):R142. doi: 10.1186/cc12821. Crit Care. 2013. PMID: 23876230 Free PMC article. Review.
-
Noninvasive mechanical ventilation in early acute respiratory distress syndrome.Pol Arch Intern Med. 2017 Sep 29;127(9):614-620. doi: 10.20452/pamw.4088. Epub 2017 Aug 17. Pol Arch Intern Med. 2017. PMID: 28820175 Review.
Cited by
-
ISCCM Guidelines for the Use of Non-invasive Ventilation in Acute Respiratory Failure in Adult ICUs.Indian J Crit Care Med. 2020 Jan;24(Suppl 1):S61-S81. doi: 10.5005/jp-journals-10071-G23186. Indian J Crit Care Med. 2020. PMID: 32205957 Free PMC article.
-
High-flow nasal oxygen in acute hypoxemic respiratory failure: A narrative review of the evidence before and after the COVID-19 pandemic.Front Med (Lausanne). 2022 Nov 25;9:1068327. doi: 10.3389/fmed.2022.1068327. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36507524 Free PMC article. Review.
-
Randomised controlled trial for high-dose intravenous zinc as adjunctive therapy in SARS-CoV-2 (COVID-19) positive critically ill patients: trial protocol.BMJ Open. 2020 Dec 2;10(12):e040580. doi: 10.1136/bmjopen-2020-040580. BMJ Open. 2020. PMID: 33268419 Free PMC article.
-
Prediction of survival time after terminal extubation: the balance between critical care unit utilization and hospice medicine in the COVID-19 pandemic era.Eur J Med Res. 2023 Jan 11;28(1):21. doi: 10.1186/s40001-022-00972-w. Eur J Med Res. 2023. PMID: 36631882 Free PMC article.
-
Management and Treatment of COVID-19: The Chinese Experience.Can J Cardiol. 2020 Jun;36(6):915-930. doi: 10.1016/j.cjca.2020.04.010. Epub 2020 Apr 17. Can J Cardiol. 2020. PMID: 32439306 Free PMC article. Review.
References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Antonelli M, Conti G, Esquinas A, Montini L, Maggiore SM, Bello G, Rocco M, Maviglia R, Pennisi MA, Gonzalez-Diaz G, et al. A multiple-center survey on the use in clinical practice of noninvasive ventilation as a first-line intervention for acute respiratory distress syndrome. Crit Care Med. 2007;35(1):18–25. doi: 10.1097/01.CCM.0000251821.44259.F3. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
