

Absolute lymphocyte count as a prognostic biomarker for overall survival in patients with advanced melanoma treated with ipilimumab
- PMID: 31425479
- PMCID: PMC7485135
- DOI: 10.1097/CMR.0000000000000633
Absolute lymphocyte count as a prognostic biomarker for overall survival in patients with advanced melanoma treated with ipilimumab
Abstract
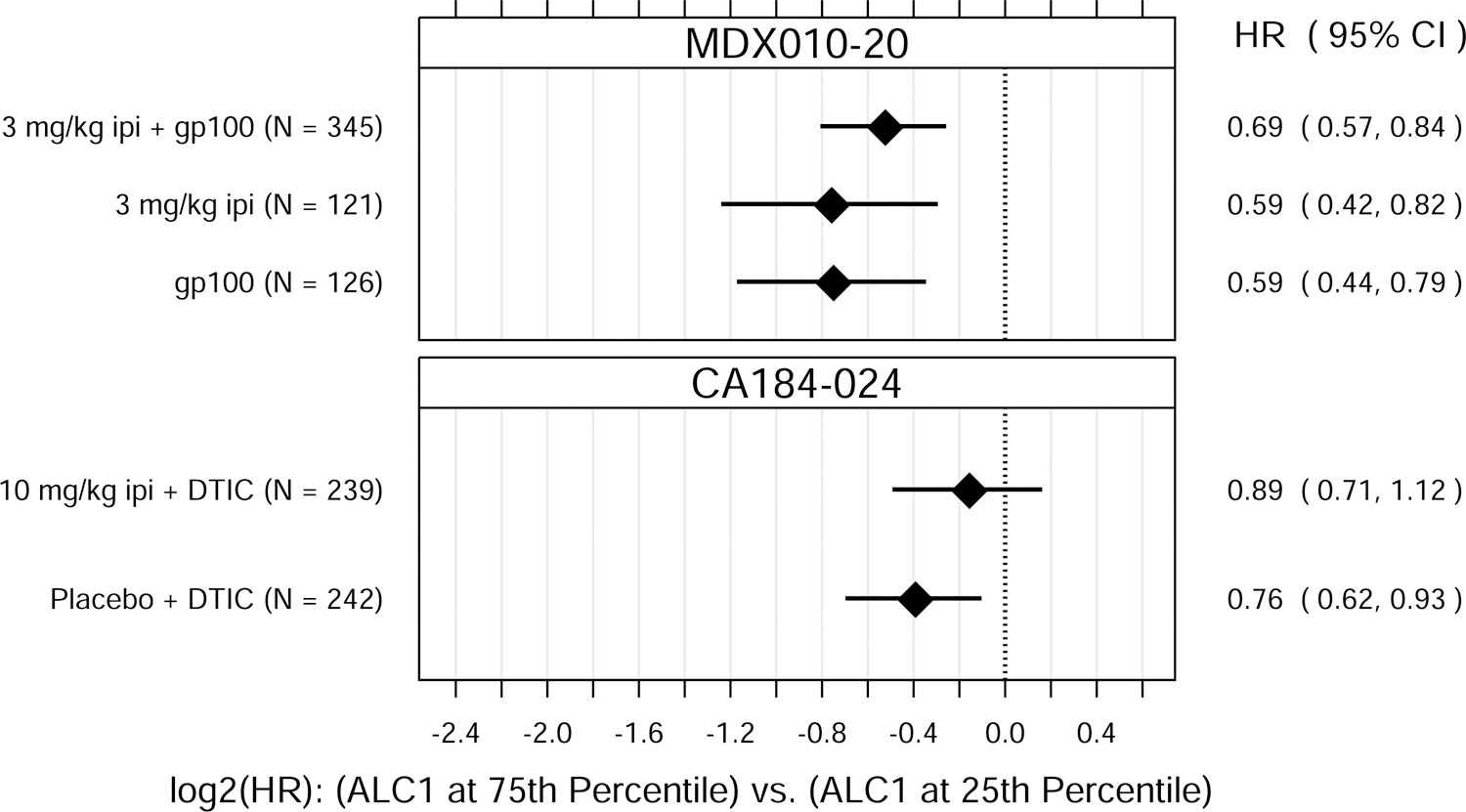
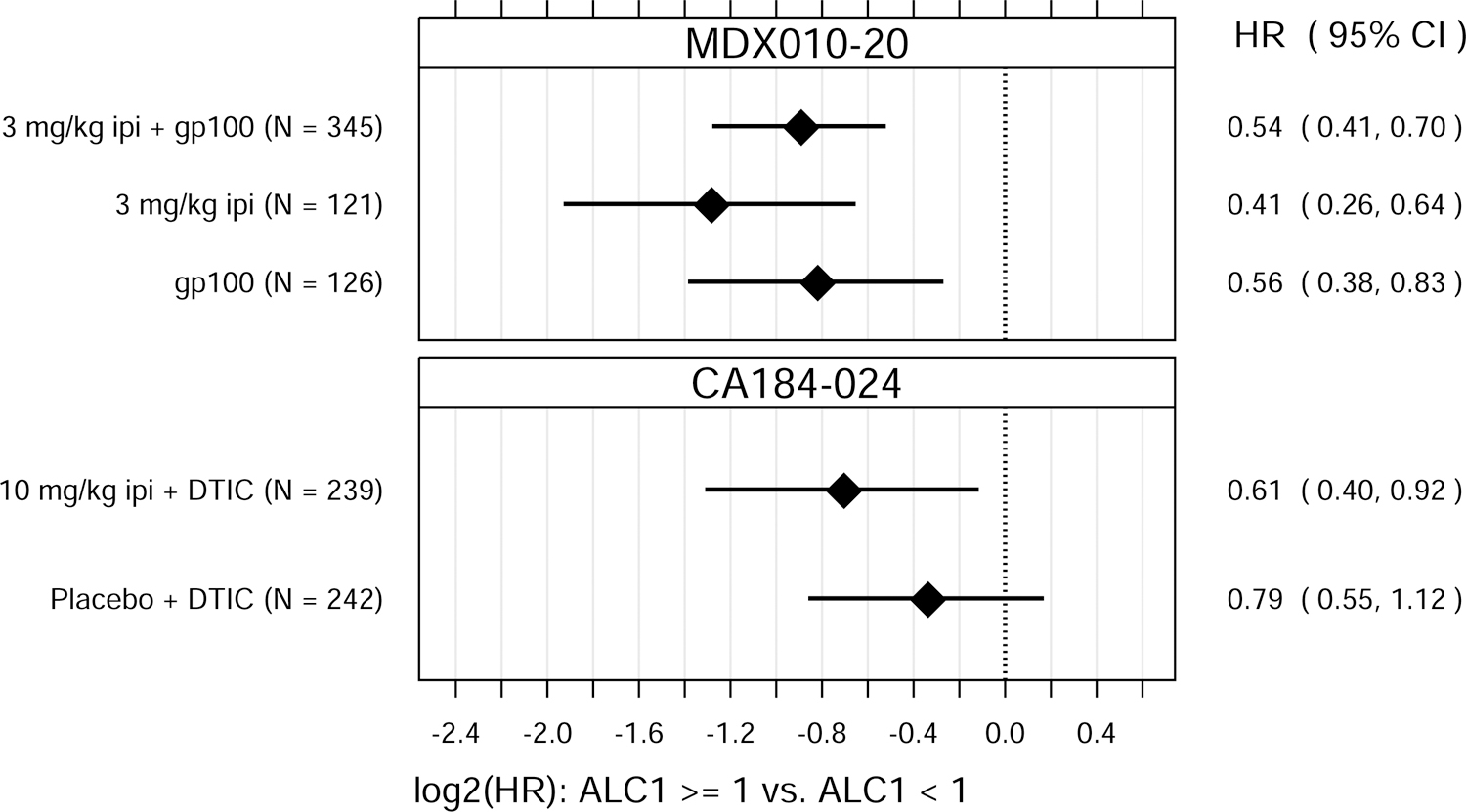
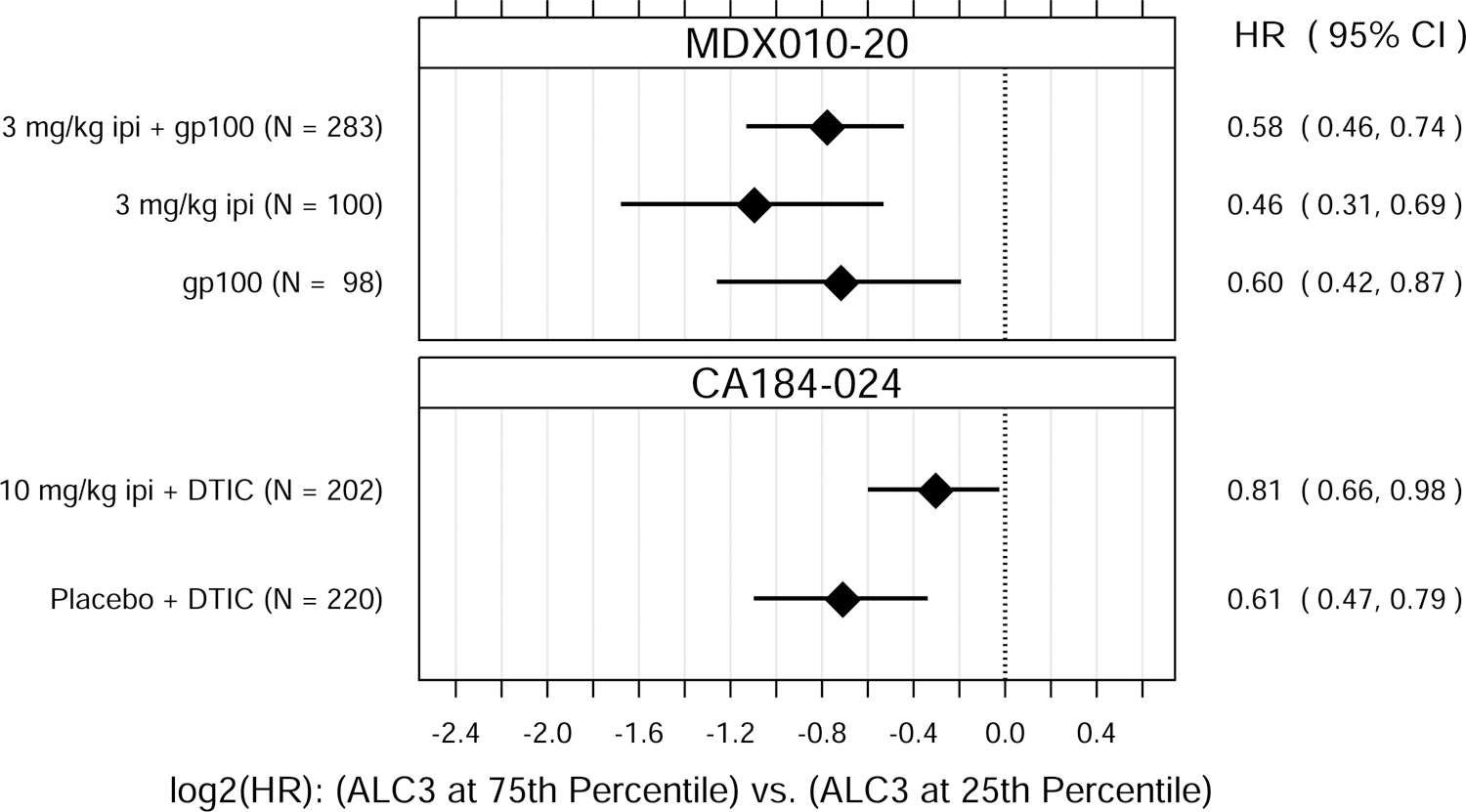
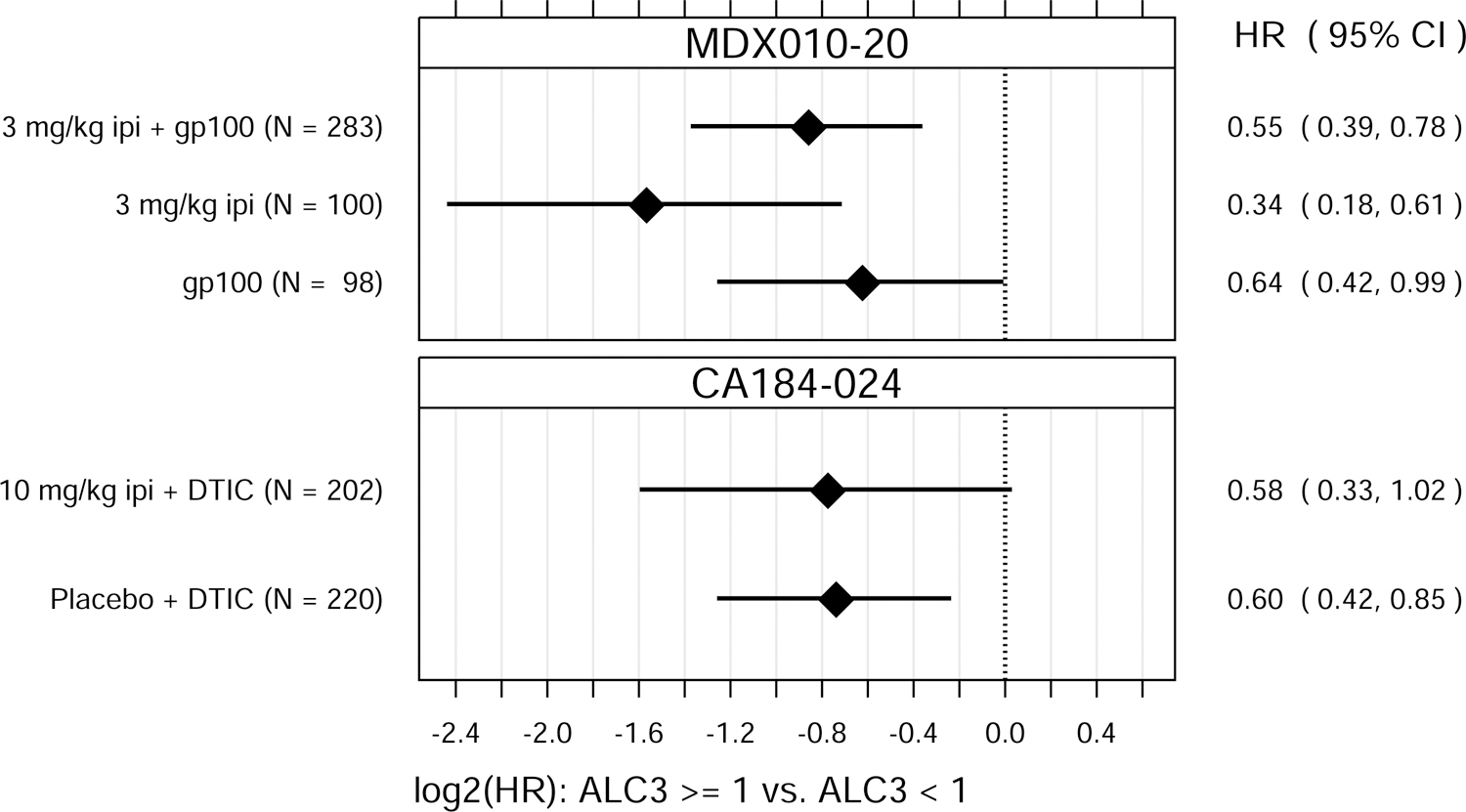
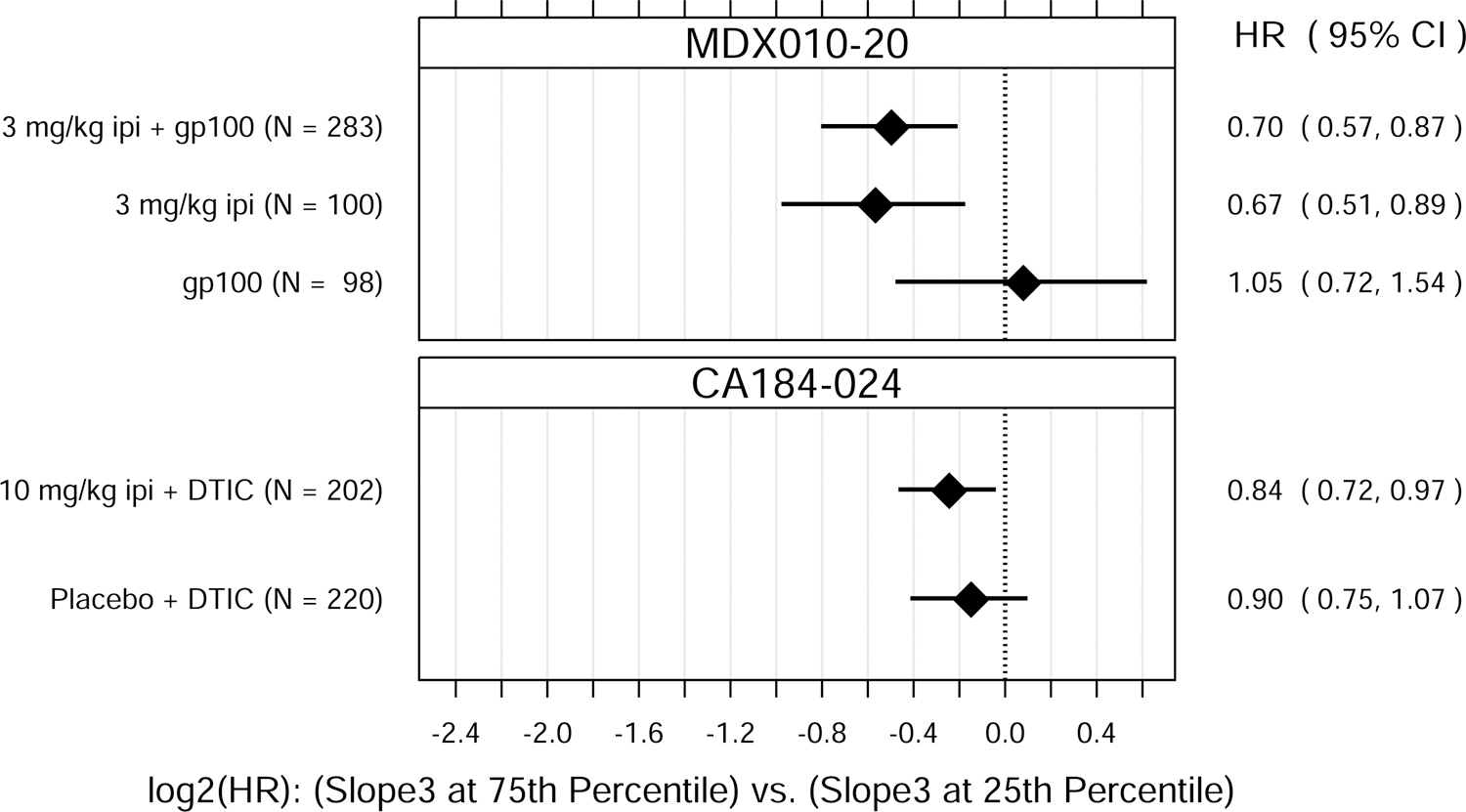
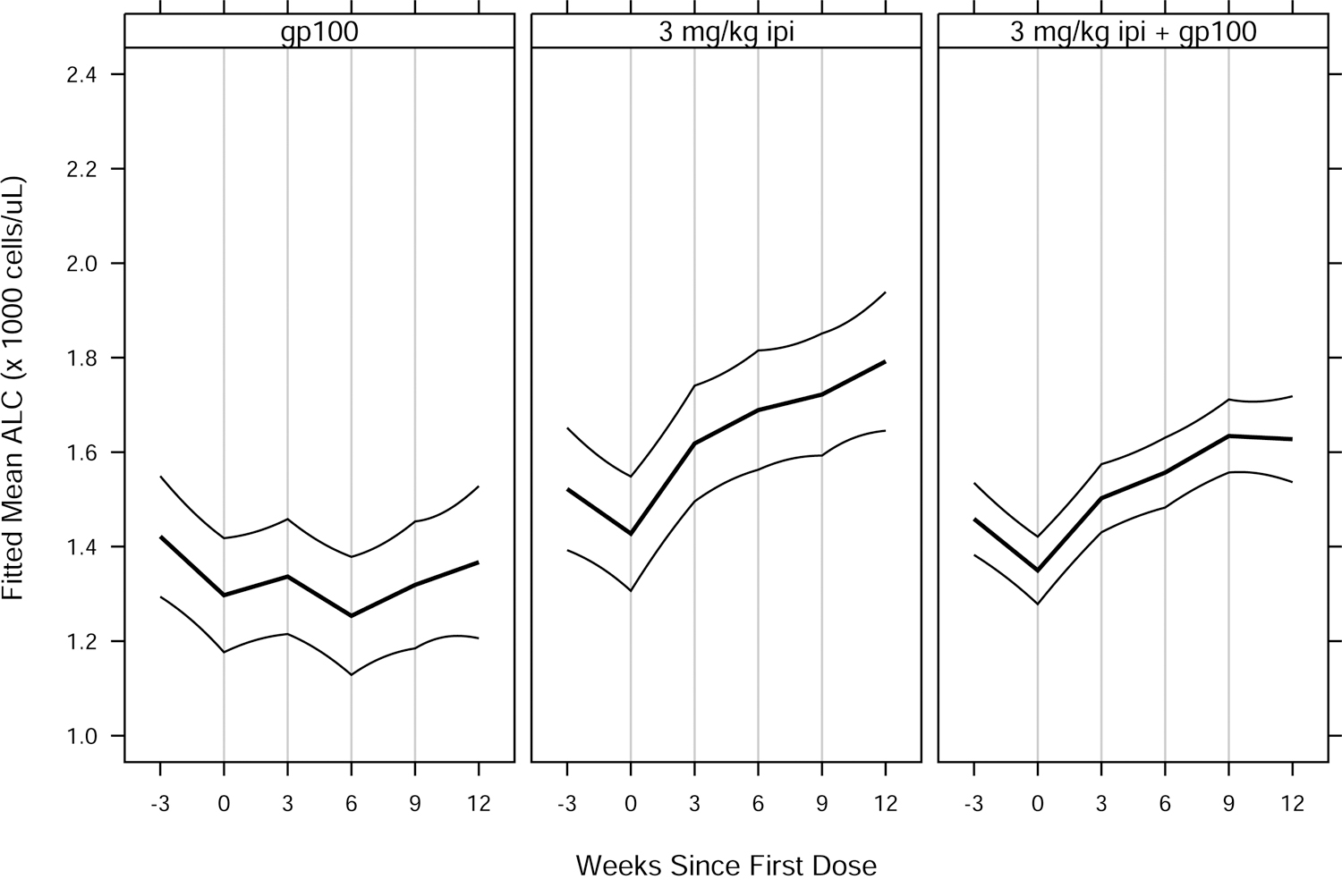
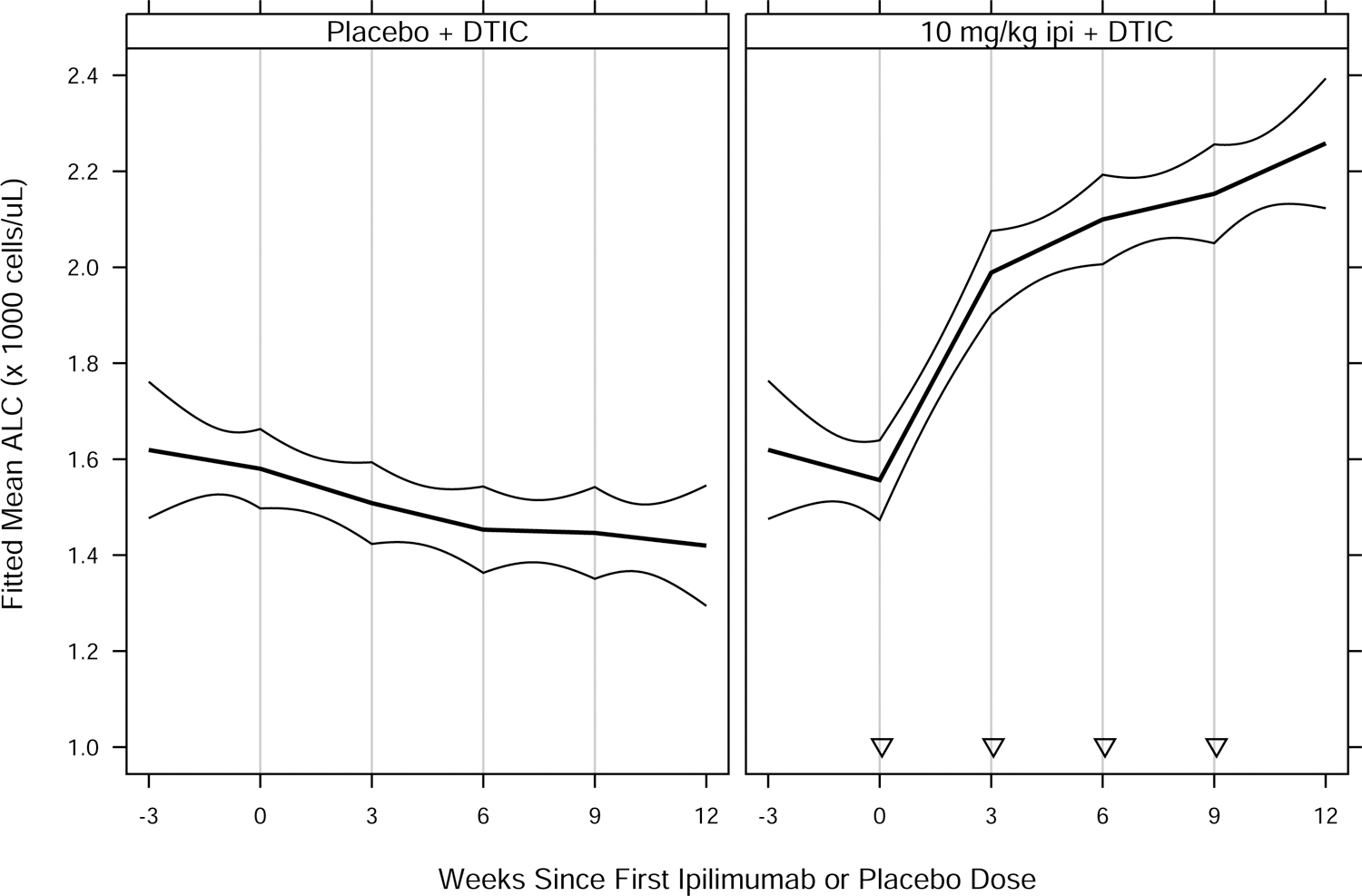
Biomarkers are needed to estimate which patients benefit most from combination ipilimumab and nivolumab immunotherapy. Rigorous biomarker analyses from prior ipilimumab randomized studies without nivolumab are likely to inform which biomarker analyses should be prioritized when examining patients treated with the combination. For the first time, the current analyses investigate absolute lymphocyte count (ALC) in randomized, controlled trials of ipilimumab without nivolumab to assess whether ALC is prognostic or predictive of ipilimumab treatment benefit. Data included patients (n = 1136) treated in the two randomized, controlled phase III studies MDX010-20 and CA184-024. ALC was measured at pretreatment baseline and every 3 weeks for up to 12 weeks, before each dose of ipilimumab. Cox proportional hazards models were used to estimate and test associations between ALC measures and overall survival (OS). In both randomized studies, baseline ALC and ALC halfway through induction (at week 6) were associated with OS not only in ipilimumab-treated patients but also in patients treated with non-ipilimumab control treatments. ALC increased in patients receiving ipilimumab, but this degree of change was not predictive of ipilimumab treatment benefit. Using data from randomized, controlled studies, we were able to conclude for the first time that baseline ALC, ALC halfway through induction (week 6) and the degree of ALC change from baseline to week 6 are prognostic biomarkers in melanoma patients, and do not appear to be predictive of ipilimumab treatment benefit. This more comprehensive understanding of ALC as a biomarker from ipilimumab trials will inform subsequent biomarker investigations in ongoing ipilimumab combination studies such as ipilimumab in combination with nivolumab.
Figures
Similar articles
-
Biomarkers Associated with Clinical Outcome of Advanced Melanoma Patients Treated with Ipilimumab.Pathol Oncol Res. 2020 Jan;26(1):317-325. doi: 10.1007/s12253-018-0466-9. Epub 2018 Sep 17. Pathol Oncol Res. 2020. PMID: 30225783
-
Investigation of clinical factors associated with longer overall survival in advanced melanoma patients treated with sequential ipilimumab.J Dermatol. 2019 Jun;46(6):498-506. doi: 10.1111/1346-8138.14865. Epub 2019 Apr 4. J Dermatol. 2019. PMID: 30945333
-
Increases in Absolute Lymphocytes and Circulating CD4+ and CD8+ T Cells Are Associated with Positive Clinical Outcome of Melanoma Patients Treated with Ipilimumab.Clin Cancer Res. 2016 Oct 1;22(19):4848-4858. doi: 10.1158/1078-0432.CCR-16-0249. Epub 2016 May 11. Clin Cancer Res. 2016. PMID: 27169993 Free PMC article.
-
Baseline Peripheral Blood Biomarkers Associated with Clinical Outcome of Advanced Melanoma Patients Treated with Ipilimumab.Clin Cancer Res. 2016 Jun 15;22(12):2908-18. doi: 10.1158/1078-0432.CCR-15-2412. Epub 2016 Jan 19. Clin Cancer Res. 2016. PMID: 26787752 Free PMC article.
-
Single-institution experience with ipilimumab in advanced melanoma patients in the compassionate use setting: lymphocyte count after 2 doses correlates with survival.Cancer. 2010 Apr 1;116(7):1767-75. doi: 10.1002/cncr.24951. Cancer. 2010. PMID: 20143434 Free PMC article.
Cited by
-
Examining the Relationship between Circulating CD4- CD8- Double-Negative T Cells and Outcomes of Immuno-Checkpoint Inhibitor Therapy-Looking for Biomarkers and Therapeutic Targets in Metastatic Melanoma.Cells. 2021 Feb 16;10(2):406. doi: 10.3390/cells10020406. Cells. 2021. PMID: 33669266 Free PMC article.
-
Current Melanoma Treatments: Where Do We Stand?Cancers (Basel). 2021 Jan 9;13(2):221. doi: 10.3390/cancers13020221. Cancers (Basel). 2021. PMID: 33435389 Free PMC article. Review.
-
Prognostic Value of Fibrinogen and Lymphocyte Count in Intermediate and High Risk Gastrointestinal Stromal Tumors.Cancer Manag Res. 2020 Sep 8;12:8149-8157. doi: 10.2147/CMAR.S262570. eCollection 2020. Cancer Manag Res. 2020. PMID: 32982412 Free PMC article.
-
Prognostic Clinical and Radiographic Biomarkers for BRAF-Targeted Therapy in Advanced Melanoma.Oncologist. 2021 Feb;26(2):e333-e335. doi: 10.1002/onco.13562. Epub 2020 Nov 4. Oncologist. 2021. PMID: 33044751 Free PMC article.
-
Predictive significance of surgery-induced lymphopenia on the survival after curative resection for locally advanced gastric cancer: a retrospective cohort analysis.World J Surg Oncol. 2023 Jan 16;21(1):7. doi: 10.1186/s12957-023-02887-0. World J Surg Oncol. 2023. PMID: 36647123 Free PMC article.
References
-
- Hodi FS, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Cowey CL, et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol 2018; 19:1480–1492. - PubMed
-
- Robert C, Thomas L, Bondarenko I, O’Day S, Weber J, Garbe C, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med 2011; 364:2517–2526. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
