

Molecular retargeting of antibodies converts immune defense against oncolytic viruses into cancer immunotherapy
- PMID: 31324774
- PMCID: PMC6642145
- DOI: 10.1038/s41467-019-11137-5
Molecular retargeting of antibodies converts immune defense against oncolytic viruses into cancer immunotherapy
Abstract
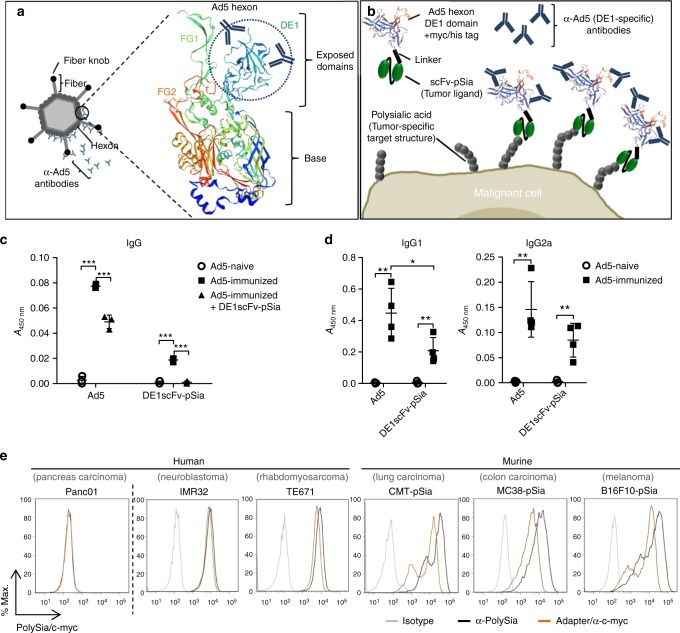
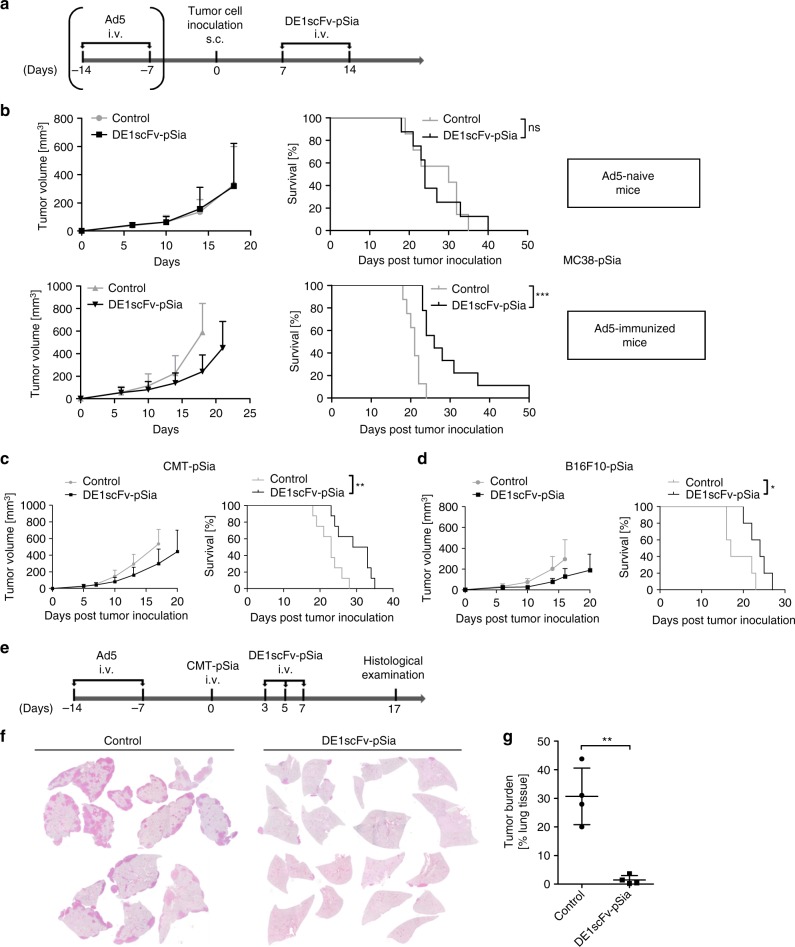
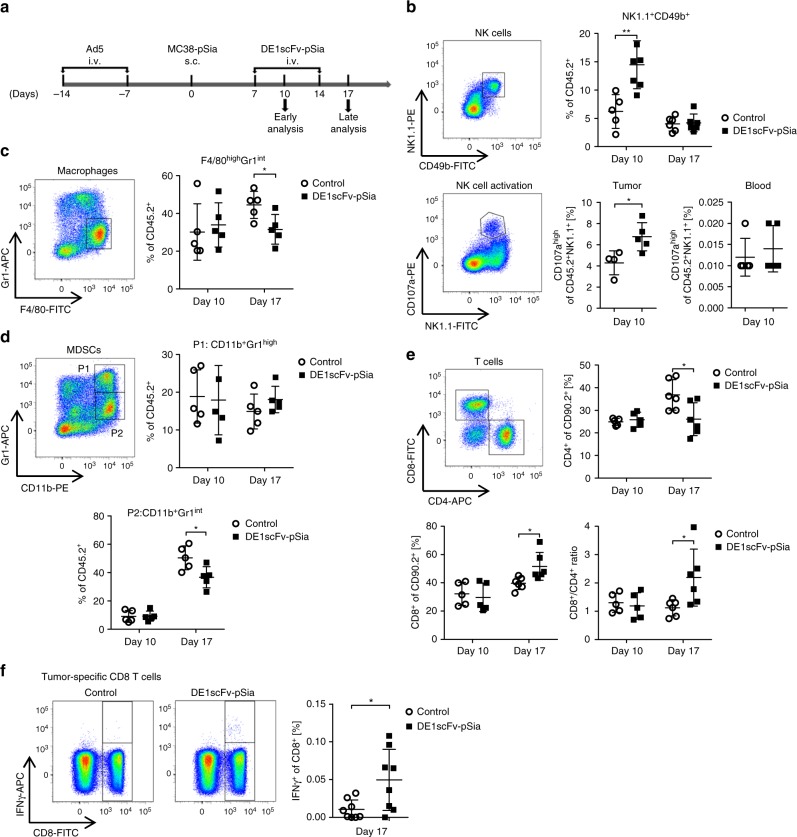
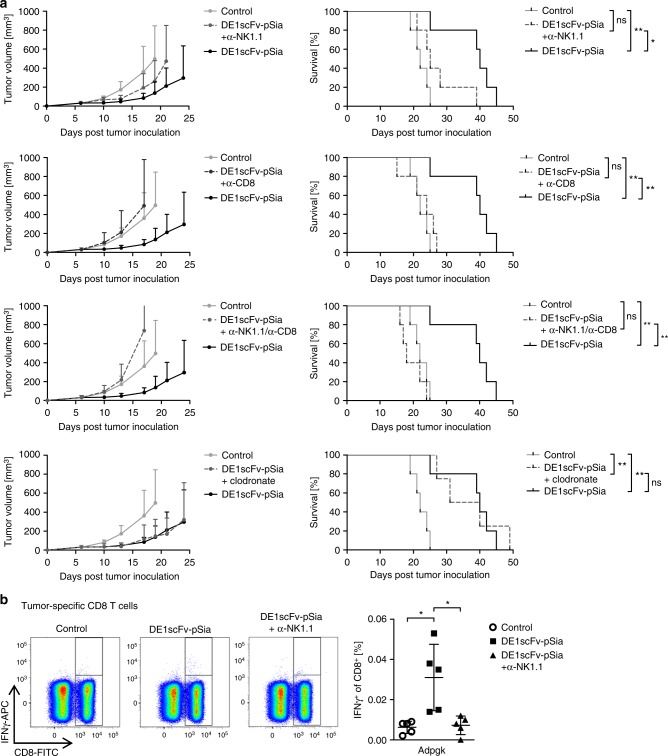
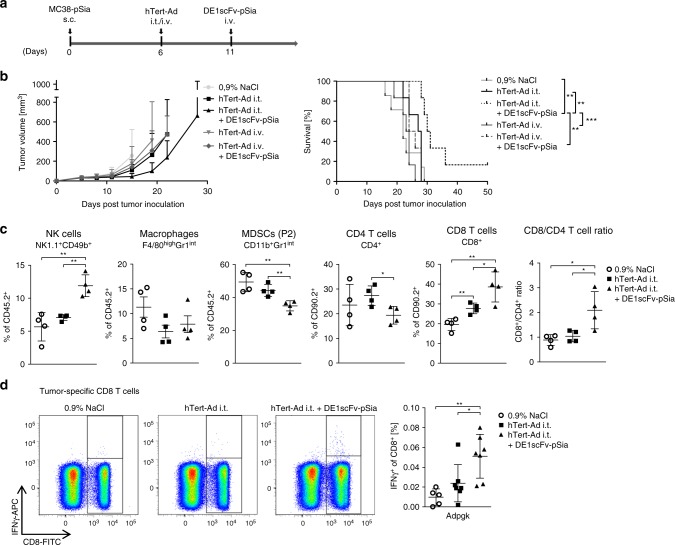
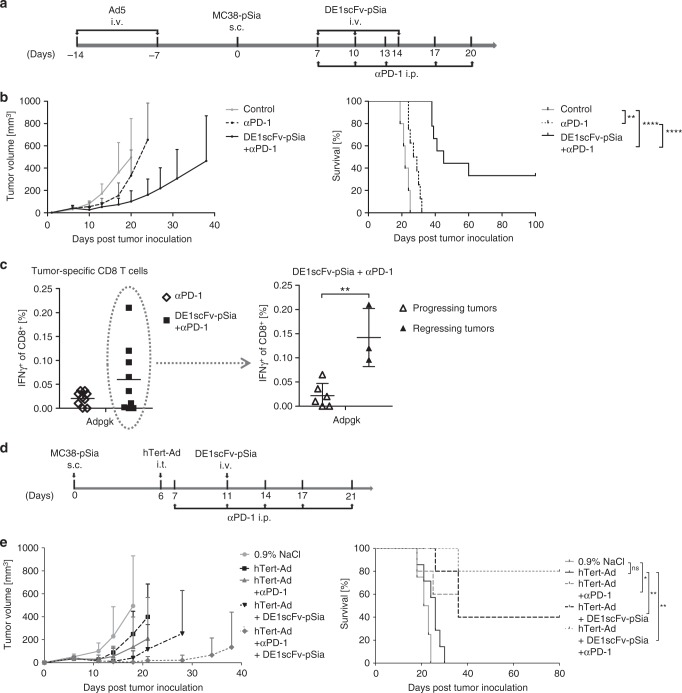
Virus-neutralizing antibodies are a severe obstacle in oncolytic virotherapy. Here, we present a strategy to convert this unfavorable immune response into an anticancer immunotherapy via molecular retargeting. Application of a bifunctional adapter harboring a tumor-specific ligand and the adenovirus hexon domain DE1 for engaging antiadenoviral antibodies, attenuates tumor growth and prolongs survival in adenovirus-immunized mice. The therapeutic benefit achieved by tumor retargeting of antiviral antibodies is largely due to NK cell-mediated triggering of tumor-directed CD8 T-cells. We further demonstrate that antibody-retargeting (Ab-retargeting) is a feasible method to sensitize tumors to PD-1 immune checkpoint blockade. In therapeutic settings, Ab-retargeting greatly improves the outcome of intratumor application of an oncolytic adenovirus and facilitates long-term survival in treated animals when combined with PD-1 checkpoint inhibition. Tumor-directed retargeting of preexisting or virotherapy-induced antiviral antibodies therefore represents a promising strategy to fully exploit the immunotherapeutic potential of oncolytic virotherapy and checkpoint inhibition.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Novel oncolytic adenovirus expressing enhanced cross-hybrid IgGA Fc PD-L1 inhibitor activates multiple immune effector populations leading to enhanced tumor killing in vitro, in vivo and with patient-derived tumor organoids.J Immunother Cancer. 2021 Aug;9(8):e003000. doi: 10.1136/jitc-2021-003000. J Immunother Cancer. 2021. PMID: 34362830 Free PMC article.
-
Immune Modulation by Telomerase-Specific Oncolytic Adenovirus Synergistically Enhances Antitumor Efficacy with Anti-PD1 Antibody.Mol Ther. 2020 Mar 4;28(3):794-804. doi: 10.1016/j.ymthe.2020.01.003. Epub 2020 Jan 10. Mol Ther. 2020. PMID: 31991110 Free PMC article.
-
Modification of oncolytic adenovirus and its application in cancer therapy.Discov Med. 2020 Nov-Dec;30(161):129-144. Discov Med. 2020. PMID: 33593481
-
Evolving Status of Clinical Immunotherapy with Oncolytic Adenovirus.Clin Cancer Res. 2021 Jun 1;27(11):2979-2988. doi: 10.1158/1078-0432.CCR-20-1565. Epub 2021 Feb 1. Clin Cancer Res. 2021. PMID: 33526422 Review.
-
Role of NK cells in immunotherapy and virotherapy of solid tumors.Immunotherapy. 2015;7(8):861-82. doi: 10.2217/imt.15.53. Epub 2015 Aug 28. Immunotherapy. 2015. PMID: 26314197 Review.
Cited by
-
CD147: an integral and potential molecule to abrogate hallmarks of cancer.Front Oncol. 2023 Nov 7;13:1238051. doi: 10.3389/fonc.2023.1238051. eCollection 2023. Front Oncol. 2023. PMID: 38023152 Free PMC article. Review.
-
A vector-encoded bispecific killer engager to harness virus-activated NK cells as anti-tumor effectors.Cell Death Dis. 2023 Feb 10;14(2):104. doi: 10.1038/s41419-023-05624-3. Cell Death Dis. 2023. PMID: 36765035 Free PMC article.
-
Adenovirus and Immunotherapy: Advancing Cancer Treatment by Combination.Cancers (Basel). 2020 May 21;12(5):1295. doi: 10.3390/cancers12051295. Cancers (Basel). 2020. PMID: 32455560 Free PMC article. Review.
-
Tutorial: design, production and testing of oncolytic viruses for cancer immunotherapy.Nat Protoc. 2024 Sep;19(9):2540-2570. doi: 10.1038/s41596-024-00985-1. Epub 2024 May 20. Nat Protoc. 2024. PMID: 38769145 Review.
-
Oncolytic Adenovirus in Cancer Immunotherapy.Cancers (Basel). 2020 Nov 13;12(11):3354. doi: 10.3390/cancers12113354. Cancers (Basel). 2020. PMID: 33202717 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
